TTFields cause disruption during mitosis leading to an asymmetric distribution of chromosomes and misalignment of metaphase plates during mitosis, (compare Figure 1A and Figure 1B). TTFields are thought to exert their effect by perturbing the function of high dipole moment possessing proteins such as α/β-tubulin or septin. One proposed model for TTFields action on mitotic cells is that they perturb septin function. Normally, septin acts to organize the cytokinetic furrow and to reinforce the structurally important interaction between the subcortical actin cytoskeleton and the overlying plasma membrane that is needed to resist intracellular hydrostatic forces produced during furrow ingression. This results in a loss of structural integrity within the dividing cells that is necessary for normal mitosis, resulting in the disruption of chromosomal segregation and cytokinetic furrow function leading to aberrant mitotic exit (Figure 1C).
Electric field intensity is not homogenous within the brain of patients undergoing TTFields treatment32. Electrical conductivity and relative permittivity of individual tissue types and their volume results in a variation of electric field intensity and distribution within the brain, shown in Figure 2A,B. Therefore, transducer array placement may have an effect on electric field strength in the region of the tumor. An example of this variability is shown in Figure 2C, which predicts the electric field strength within the patient's brain at adjacent axial, coronal, and sagittal slices.
Figure 3A shows the personalized output of the treatment planning software for the proper placement of the arrays on a patient, shown in Figure 3B. Scalp sensitivity to the arrays can be alleviated by topical application of corticosteroids and by shifting the arrays as described in Figure 4.
The above protocol was used to treat a 56-year-old woman who developed a hemorrhage in the left frontal brain. She underwent a gross total resection of the hemorrhagic mass and the pathology showed IDH-1 mutated glioblastoma with hypercellularity, cellular atypia, mitotic figures and necrosis. She subsequently received external beam radiotherapy and daily temozolomide. Dexamethasone was stopped early at the second week of radiation. She experienced pancytopenia due to temozolomide administered during the adjuvant phase of treatment, requiring growth factor support as well as platelet and blood transfusions. Increased gadolinium enhancement was noted on head MRI 5 months after diagnosis and bevacizumab was started. Eight months after diagnosis TTFields therapy was also added. She has been maintained on the regimen of bevacizumab and TTFields for 48+ months after the diagnosis of her glioblastoma. The MRI images of this patient revealed stable disease for 48 months after initial diagnosis of glioblalstoma, shown in Figure 5. She has survived thus far with a high Karnofsky score of 80.
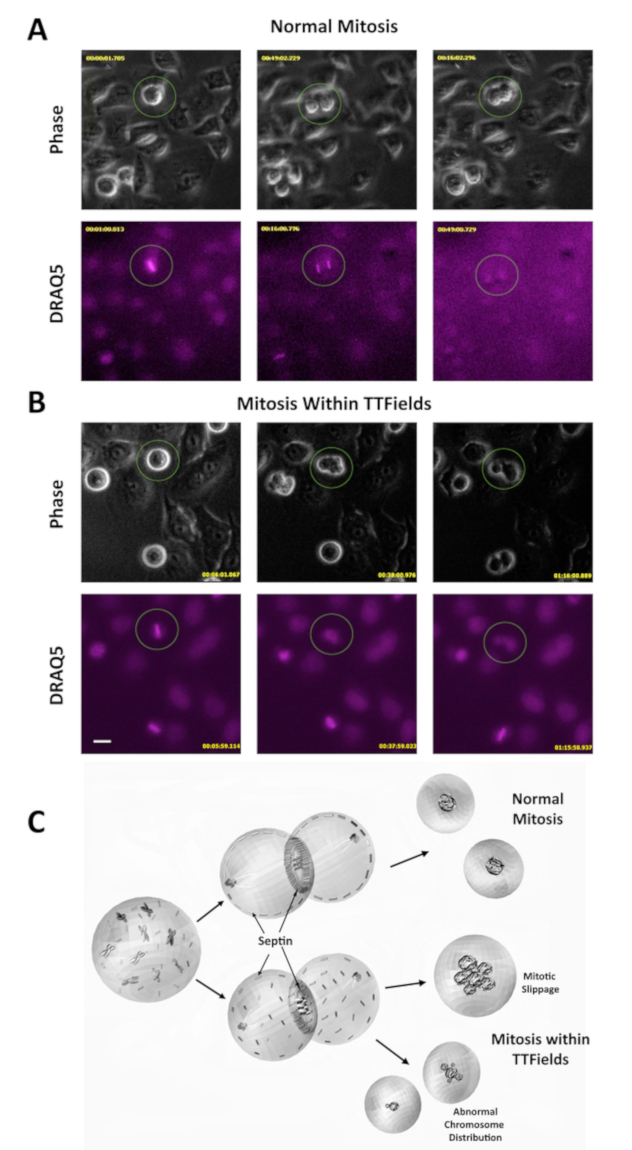
Figure 1: TTFields disrupt mitosis during cell division. (A) Phase contrast microscopy was used to observe HeLa cells during mitosis. DRAQ5 is a DNA stain and was used to monitor chromosomal behavior. Image taken from a video of cells undergoing normal mitosis, included as an additional supplement. The procedures for obtaining video images were described in previous work11. (B) Phase contrast and DRAQ5 under TTFields show cell blebbing and aberrant mitosis. Scale bar = 20 µm. Image taken from a video of cells undergoing mitosis during TTFields treatment, included as an additional supplement. The procedures for obtaining video images were described in previous work11. (C) Proposed model for TTFields-induced mitotic disruption. TTFields perturb septin association with the cytokinetic furrow and the subcortical actin cytoskeleton. This creates insufficient furrow contractility and makes cells vulnerable to plasma membrane rupture from the underlying cytoskeleton, resulting in membrane blebbing. This leads to aberrant mitotic exit including mitotic slippage (failure to divide) and asymmetric cell division. Please click here to view a larger version of this figure.
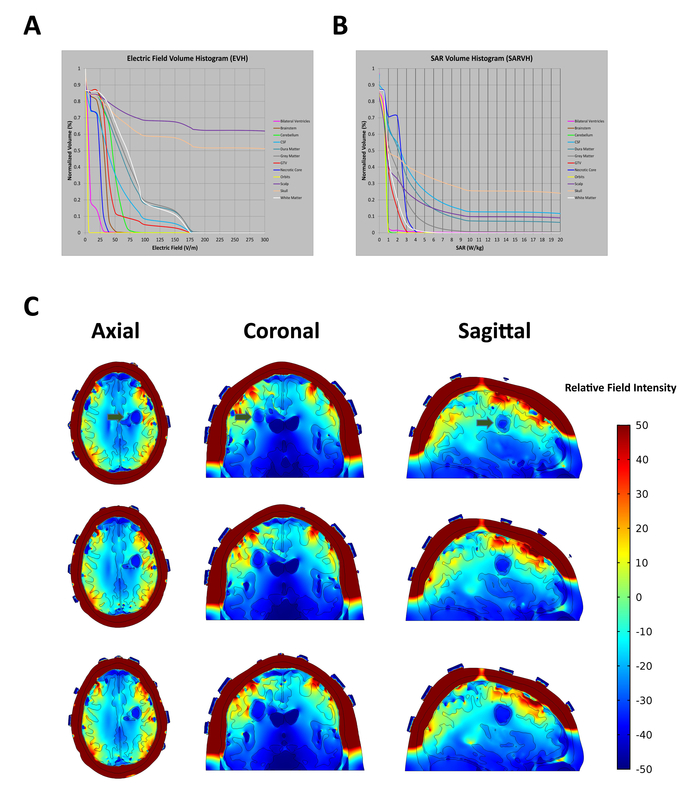
Figure 2: In situ electric field intensities vary within tissues based on electric conductivity and relative permittivity of the tissues they pass through. (A) Electric Field-Volume Histogram (EVH) shows the magnitude of electric field strength. (B) Specific Absorption Rate-Volume histogram (SARVH) shows the rate of energy absorbed in different tissues. (C) Representative field mapping of a patient with a left frontal glioblastoma, showing field strength within distributions on axial, coronal and sagittal slices. Green arrows indicate location of tumor. Relative electric field intensity is arbitrary. Please click here to view a larger version of this figure.
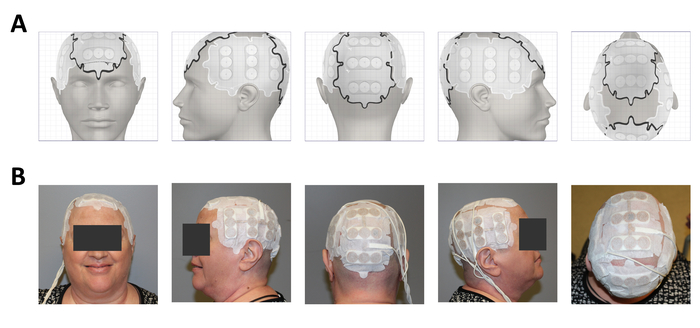
Figure 3: Clinical application on a glioblastoma patient after surgery, radiation and temozolomide. (A) Treatment planning software output showing placement of the 4 arrays. (B) Array placement on the patient. Please click here to view a larger version of this figure.
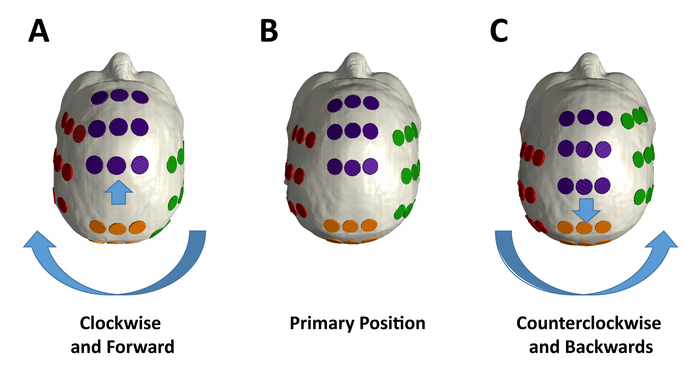
Figure 4: Array placement variation during treatment. (A) The individual lateral arrays should be rotated in aggregate by 2 cm from their primary position in a clockwise fashion, and the frontal and posterior arrays moved forward by 2 cm from the (B) primary positions for array placement position, which are based on the output from the treatment planning software for the individual patient. (C) The individual electrodes in each array should be rotated in aggregate by 2 cm from the primary position in a counterclockwise fashion, and the anterior and posterior arrays moved in aggregate by 2 cm backwards. Please click here to view a larger version of this figure.
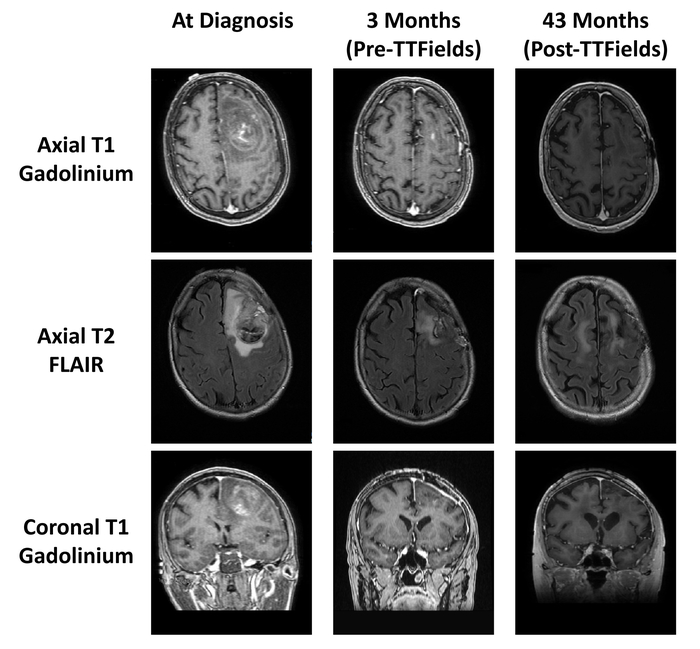
Figure 5: Patient MRI scans before and after TTFields treatment. MRI scans at diagnosis (left column), MRI scans after surgery, radiation, and temozolomide (middle column), and MRI scans after 43 months of TTFields treatment (right column). Please click here to view a larger version of this figure.
