Portable pupillometer devices are produced by several companies. These devices are typically conveniently sized and can be operated with one hand (Figure 1A), enabling examiners to accurately detect pupillary responses by pressing a button. Infrared light is used to detect the pupillary edge automatically (Figure 1B), accurately representing pupillary data (Figure 1C). This device measures maximum (initial) resting pupil size (MAX), minimum pupil size after stimulation (MIN), constriction pupil size ratio (%constriction, [MAX-MIN]/MAX expressed as a percentage), latency duration (LAT, time between initiation of retinal light stimulation and onset of pupillary constriction), constriction velocity (CV, extent of constriction/duration of constriction), maximum constriction velocity (MCV), dilation velocity (DV, extent of pupil size recovery/duration of recovery). The light reflex is acquired using a flash of visible white light of 800 ms duration at the start of each 3.2 s scan11. We report the relationship between the pupillary response and efficacy of ECT using this device among 13 patients (Figure 3, this figure has been modified from reprinted from Shirozu et al.9. As shown in Figure 3A, pupillary diameter was increased after electrical stimulation. However, significant differences in constriction by the light reflex were caused immediately after electrical stimulation, reflecting differences in seizure efficacy induced by ECT (Figure 3B).
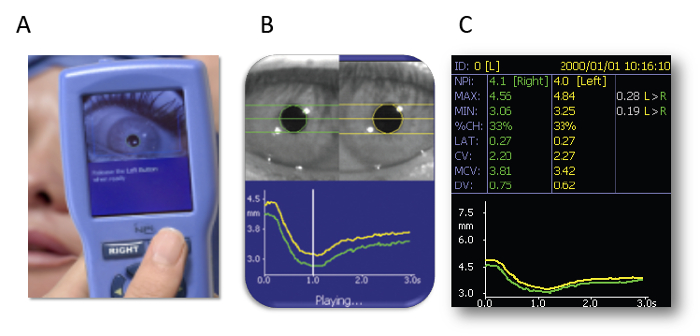
Figure 1: Automated infrared pupillometer. (A) The measurement method. (B) Detecting the edge of the pupil. (C) Representing the pupillary data. The images are presented with the explicit permission from the commercial supplier. Please click here to view a larger version of this figure.
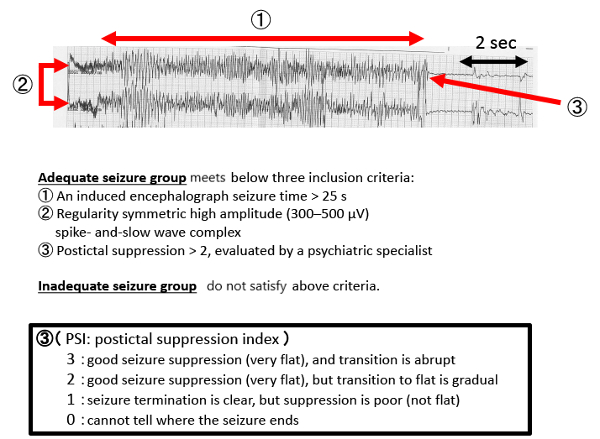
Figure 2: EEG results during a typical seizure. Please click here to view a larger version of this figure.
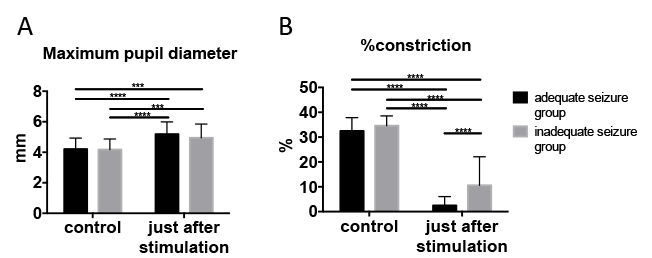
Figure 3: Pupillary response changed immediately after electrical stimulation. (A) Maximum pupil diameter. (B) Pupillary constriction ratio (light reflex). We used two-way ANOVA for comparisons between adequate and inadequate seizure groups at control, and just after stimulation. Adequate seizure status was determined using the criteria described above. Data are presented as mean ± standard deviation. Sidak’s multiple-comparison post hoc test was utilized for two-way analysis of variance. ***p < 0.001, ****p < 0.0001. This figure has been modified from reprinted from Shirozu et al.9 with permission. Please click here to view a larger version of this figure.
