Using the procedure presented here, we treated eyes with a Nd:YAG laser, evaluating different pulse energies (1.0−4.6 mJ) and positions of focal points (distance from the posterior surface of the cornea: 0.0−0.2 mm) to find the optimal parameters. Multiple replicates (n = 3) were evaluated for each constellation of the laser parameters (12 x 21).
In addition to the above-mentioned protocol, specimen was analyzed with a two-photon microscope before fixation and H&E staining. The two-photon microscope used a solid-state, mode-locked 80 MHz Ti:sapphire laser with a tuning range of 690−1b040 nm and a mean laser output of >900 mW at 800 nm as light source. It delivered pulses with a width of approximately 150 fs to the sample. Images were taken with a microscope objective (20x/0.95) at a wavelength of 730 nm and 30 mW of laser power.
Two-photon as well as light microscopy images were independently reviewed by 3 reviewers, who were blinded to experimental settings and had to assign the images to three categories: (1) no damage, (2) too much damage, or (3) right amount of damage (Figure 2 and Figure 3). Based on their evaluation a heatmap was calculated (Figure 4). Using this heatmap it is possible to select the right constellation of laser parameters to selectively ablate CEC with minimal damage to surrounding tissue (green). Results show that the focal point of the laser must be at least 0.15 mm behind the corneal endothelium for the lowest pulse energy (1.0 mJ) tested. For pulse energies higher than 2.9 mJ, the longest focal distance tested (0.2 mm) is still too close to the endothelium.
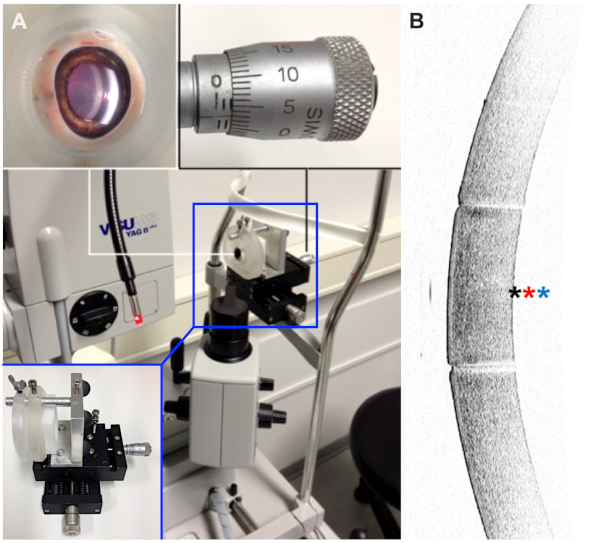
Figure 1: Experimental setup. (A) Eyes were fixed in a partially 3D-printed holding apparatus, which allowed precise alignment with respect to the laser beam. (B) Before laser treatment, the tissue was evaluated with an anterior segment optical coherence tomography device to check for major anterior segment pathologies. Positions of focal laser points are indicated with exemplary for 0.0 mm (black asterisk), 0.1 mm (red asterisk), and 0.2 mm (blue asterisk). Please click here to view a larger version of this figure.
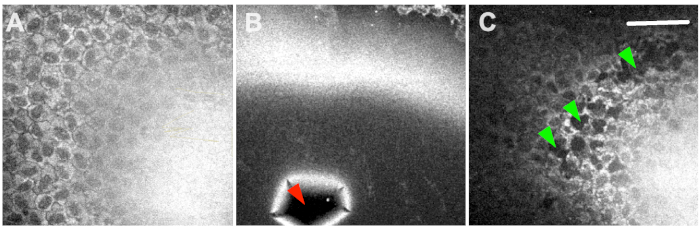
Figure 2: Two-photon microscopy. Results ranged from no damage at all (A), extensive collateral damage (B) to selective ablation of endothelial cells (C). The red arrowhead shows a ruptured Descemet’s membrane, and green arrowheads indicate selective ablation of CEC-clusters. Scale bar = 100 µm. Please click here to view a larger version of this figure.
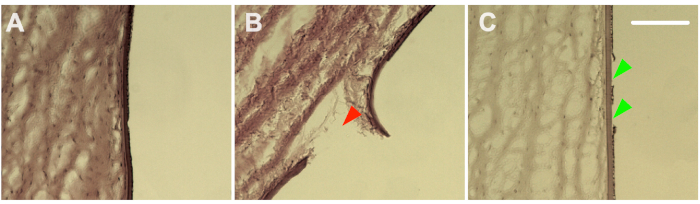
Figure 3: Histology. Hematoxylin and eosin staining confirmed the damage range from no damage at all (A), extensive collateral damage (B) to selective ablation of endothelial cells (C). The red arrowhead shows a ruptured Descemet’s membrane, and green arrowheads indicate selective ablation of CEC-clusters. Scale bar = 100 µm. Please click here to view a larger version of this figure.
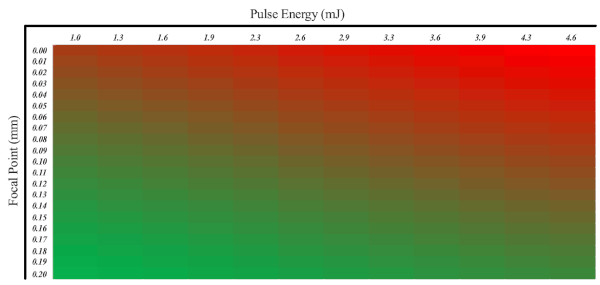
Figure 4: A heatmap showing the probability of selective CEC damage. In this regard, the pulse energy as well as the position of the Nd:YAG laser focal point must be taken into account. Excessive damage is shown in red, and the desired portion of damage is shown in green. Please click here to view a larger version of this figure.
