A Rabbit Venous Interposition Model Mimicking Revascularization Surgery using Vein Grafts to Assess Intimal Hyperplasia under Arterial Blood Pressure
Summary
The present protocol aims to experimentally create venous intimal hyperplasia by subjecting veins to arterial blood pressure for developing strategies to attenuate venous intimal hyperplasia following revascularization surgery using vein grafts.
Abstract
Although vein grafts have been commonly used as autologous grafts in revascularization surgeries for ischemic diseases, the long-term patency remains poor because of the acceleration of intimal hyperplasia due to the exposure to arterial blood pressure. The present protocol is designed for the establishment of experimental venous intimal hyperplasia by interposing rabbit jugular veins to the ipsilateral carotid arteries. The protocol does not require surgical procedures deep in the body trunk and the extent of the incision is limited, which is less invasive for the animals, allowing long-term observation after implantation. This simple procedure enables researchers to investigate strategies to attenuate the progression of intimal hyperplasia of the implanted vein grafts. Using this protocol, we reported the effects transduction of microRNA-145 (miR-145), which is known to control the phenotype of vascular smooth muscle cells (VSMCs) from the proliferative to the contractile state, into harvested vein grafts. We confirmed the attenuation of intimal hyperplasia of vein grafts by transducing miR-145 before implantation surgery through the phenotype change of the VSMCs. Here we report a less invasive experimental platform to investigate the strategies that can be used to attenuate intimal hyperplasia of vein grafts in revascularization surgeries.
Introduction
The number of patients experiencing ischemic diseases due to atherosclerosis is increasing worldwide1. Despite the current advances in medical and surgical therapies for cardiovascular diseases, ischemic heart diseases, such as myocardial infarction, remain a major cause of morbidity and mortality2. Furthermore, peripheral arterial diseases characterized by reduced blood flow to the limbs induces critical limb ischemia, wherein approximately 40% of the patients lose their legs within 6 months of diagnosis, and the mortality rate is up to 20%3.
Revascularization surgeries, such as coronary artery bypass grafting (CABG) and bypass surgery for peripheral arteries, are major therapeutic options for ischemic diseases. The purpose of these surgeries is to provide a new blood pathway to provide sufficient blood flow toward the distal site of the stenotic or occluded lesions of the atherosclerotic arteries. Although in situ arterial grafts, such as internal thoracic arteries for CABG, are preferred as the bypass grafts because of the expected longer patency, vein grafts, such as autologous saphenous veins, are commonly used because of the higher accessibility and availability4. The weak point of the vein grafts is the poor patency rate compared to that of artery grafts5 due to accelerated intimal hyperplasia when subjected to arterial pressure, which leads to vein graft disease6.
Vein graft disease develops through the following three steps: 1) thrombosis; 2) intimal hyperplasia; and 3) atherosclerosis7. In order to address vein graft disease, a lot of basic research has been conducted8. Thus far, no pharmacological strategy other than antiplatelet and lipid-lowering therapies are recommended for secondary prevention after coronary or peripheral revascularization surgeries in recent guidelines9,10,11,12. Thus, to overcome vein graft disease, especially intimal hyperplasia, the establishment of a relevant experimental platform for further studies is required.
Intimal hyperplasia is an adaptive phenomenon that occurs in response to the change in the surroundings, where vascular smooth muscle cells (VSMCs) proliferate, accumulate, and generate extracellular matrix in the intima. Consequently, it presents a foundation for graft atheroma7. In the hyperplastic intima, VSMCs bear proliferation, and production rather than contraction, termed “phenotypic change”8. It is a key research target to control the phenotype of the VSMCs of the vein grafts to prevent vein graft disease, and numerous basic studies have been conducted on this topic8. However, a randomized controlled clinical study that aimed to achieve pharmacological control of the VSMC phenotype showed limited results13. Further, there are no standardized therapies to prevent intimal hyperplasia. More basic research, including animal model studies, is necessary.
To promote research in this field, it is crucial to establish an animal model that recapitulates vein grafts under arterial blood pressure, allowing a long-term, postoperative observation. Carrel et al. established a canine model of implantation of the external jugular vein into the carotid artery14. Therafter, a variety of vein grafts have been employed to investigate the physiological and pathological effects of alterations in arterial blood pressure, including the inferior vena cava engrafted into the thoracic or the abdominal aorta, or the saphenous vein engrafted into the femoral artery15,16,17. These models were built in larger animals, such as pigs or dogs, that are suitable for mimicking a vein graft disease in a clinical case. However, the establishment of an animal model that can be prepared without special surgical techniques and at a lower cost would be ideal for researchers trying to develop a new therapeutic strategy for attenuating intimal hyperplasia through VSMC phenotype control in vivo. Initially, the interposition of the jugular vein into the carotid artery in a rabbit was introduced in the field of neurosurgery18,19. Thereafter, it was applied to research on intimal hyperplasia20,21. The initial model consists of venous interposition alone, thus saving time. Moreover, a subsequent study demonstrated that the preparation of a vein graft also affected the intimal hyperplasia22. Davies et al. evaluated the effect of balloon catheter injury on the intimal hyperplasia in a rabbit venous interposition model23,24. Although balloon catheter injury in addition to vein interposition was more relevant to a clinical setting, a more reproducible model was also desired. Thus, Jiang et al. examined the impact of differential flow environments on intimal hyperplasia and established a distal branch ligation procedure as a reproducible model25. However, they employed a cuff technique at the time of vein graft interposition that seems different from hand-sewn anastomosis in the clinical setting. In the present protocol, we report a reproducible, clinically relevant, and broadly available procedure for the preparation of a rabbit venous interposition model to assess intimal hyperplasia under arterial blood pressure.
Protocol
NOTE: All the surgical procedures performed on animals should be carried out in accordance with the Guide for the Care and Use of Laboratory Animals (www.nap.edu/catalog/5140.html) or other appropriate ethical guidelines. Protocols should be approved by the animal welfare committee at the appropriate institution before proceeding.
1. Preparation of animals
- Purchase male Japanese white rabbits (or rabbits with equivalent body size) weighing 2.7–3.0 kg.
- Acclimate the rabbits for 1 week in a 12 hour light–dark cycle and feed a regular rabbit chow diet before the procedure.
2. Anesthesia and animal setting
NOTE: All the subsequent procedures must be performed under aseptic conditions. The surgical field and devices should be disinfected with 10% povidone-iodine solution, 70% alcohol, or a quaternary ammonium compound before use.
- Anesthetize a rabbit with intravenous administration of pentobarbital sodium (25 mg/kg) via the auricular vein.
- After ensuring that the rabbit has lost its strength, transfer it to an operating table, and set it in the supine position. Cover the nose and mouth with an anesthetic mask. Start the administration of general anesthesia with the inhalation of 0.7–1.0% isoflurane-oxygen mix.
NOTE: If the rabbit starts to move, a temporal surge in isoflurane up to 2% will be effective. - Trim the fur on the neck and shoulder using an electric hair clipper. After disinfecting the surface by spraying 70% ethanol or another antiseptic solution, shave the rest of the hair in the cervical region with a razor. Disinfect the surgical field with 10% povidone-iodine and administer lidocaine hydrochloride (3 mg/kg) subcutaneously as local anesthesia.
NOTE: Examine the repetitive movement of the trachea. Observe the pulsation of the jugular vein and the carotid artery. When the respiratory and pulsatile rates decrease, consider a temporary reduction in anesthesia administration. Monitoring the percutaneous oxygen saturation and pulse rate is also helpful.
NOTE: The protocol can be paused here.
3. Harvest of the jugular vein
NOTE: Local anesthetics (such as lidocaine) should be used before making the skin incision.
- Before skin incision, administer prophylactic enrofloxacin (5 mg/kg) subcutaneously. For analgesia, administer 0.05 mg/kg of buprenorphine subcutaneously twice a day for 3 days.
NOTE: To avoid a drop in body temperature, a surgical scrub of the incision site can be used instead of spraying the animal's body with 70% ethanol. - Incise 50–60 mm of the cervical region with surgical scalpel longitudinally. Bluntly dissect the subcutaneous tissues and fascia to expose a 20–30 mm segment of the jugular vein. Ligate all the branches of the exposed vein with 4-0 silk sutures.
- Place a 2-0 silk suture around the internal and external jugular veins to perform ligation immediately after incising the jugular vein in the next step.
- Incise the venous wall (approximately 1 mm) of the distal side of the vein. Insert a 2-French balloon catheter from the cut toward the proximal side of the vein. Ligate the 2-0 silk suture at the distal sites of the jugular veins.
- Inflate the balloon with 0.2 mL of air. Denude the intima of the vein using three passages of the catheter for endothelial exfoliation.
NOTE: This procedure is considered equivalent to the distension of a saphenous vein graft in human revascularization surgeries, which causes endothelial exfoliation. - Ligate the proximal end of the vein. Cut the vein to harvest.
NOTE: Carefully distinguish the distal and proximal end of the harvested vein, because the anastomosis to the artery should be performed in an inverted manner (i.e., the distal end of the vein should be anastomosed to the proximal end of the artery). For example, insertion of an intravenous catheter from a certain side would work as a marker. - For therapeutic manipulations for the harvested jugular vein, treat the harvested vein with methods designed for each research question (e.g., electroporation26 or direct immersion with solutions27 for transducing microRNAs into the veins).
NOTE: For this protocol, the vein grafts were soaked in phosphate-buffered saline, control microRNA, and microRNA-145. The protocol can be paused here.
4. Interposing the carotid artery by the harvested jugular vein
- Expose a 20–30 mm segment of the ipsilateral carotid artery. Separate the artery carefully from the vein and nerve nearby. Ligate all the branches of the exposed vein with 4-0 silk suture.
- Administer heparin sodium intravenously (200 IU/kg). Wait for 3–4 min.
- Clamp the proximal and distal ends of the artery with surgical clamps. Cut the artery in the middle, between the clamps. Inject normal saline into the incised carotid artery proximally and distally to distend the artery.
NOTE: A rabbit carotid artery tends to shrink. Choose a well-distended site as an anastomosis site. - Anastomose the harvested vein to the artery in a reversed end-to-end fashion.
- Insert a 20 G intravenous catheter into the harvested vein from the distal to the proximal direction to keep the venous lumen open during the distal anastomosis.
- Anastomose the proximal end of the vein to the distal end of the artery using 8-0 polypropylene interrupted sutures. Place two anchor stiches at the site and the opposite site. Add stiches the upper side of the anastomosis line between the anchor stiches.
- Flip the artery and the vein graft upside down. Add stiches on the remaining part of the anastomosis line.
- Remove the intravenous catheter from the vein. Clamp the vein graft proximally and declamp the carotid artery distally. Ascertain that the vein graft is expanding gradually.
- Anastomose the distal end of the vein to the proximal end of artery using 8-0 polypropylene interrupted sutures. Declamp the artery to check the bleeding from the anastomosis sites. Add sutures for hemostasis, if required.
NOTE: A gentle compression of the bleeding site with gauze and waiting may be enough for hemostasis. Check the immediate expansion and strong pulsation of the vein graft after the proximal declamping. If that is not observed, consider repeating steps 4.4.2–4.4.3
- Ligate the internal carotid artery with a 4-0 silk suture to simulate a poor runoff condition and to facilitate intimal hyperplasia.
- Clean the wound with saline. Close the wound using 3-0 polyglactin 910, layer by layer.
5. Postoperative procedures
- End the anesthesia and remove the anesthesia mask after checking the spontaneous breathing of the animal. Check the conditions of the animal frequently until it recovers from anesthesia.
- Keep the animal separated from other animals until respiratory function is fully restored. Support breathing manually, if necessary. Do not return the animal to a larger group until full recovery.
- Check the food and water intake after recovery from anesthesia and provide appropriate nutritional support. Administer analgesics (e.g., buprenorphine 0.05–0.2 mg/kg subcutaneously 2x a day for 3 days) and check for signs of discomfort or pain.
Representative Results
Figure 1A shows a representative image of successful intimal hyperplasia at 2 weeks after venous interposition surgery (upper panel). The lower panel shows the therapeutic effects of microRNA-145-loaded poly(lactic-co-glycolic acid) nanoparticles that attenuated the intimal hyperplasia (lower panel). Figure 1B shows the comparison of intimal hyperplasia between the control group using phosphate buffered saline control (PBS), control microRNA (Cont-miR), and microRNA-145 (miR-145) groups. MicroRNAs were loaded with poly(lactic-co-glycolic acid) nanoparticles. Treatment with microRNA-145 significantly attenuated intimal hyperplasia. Figure 2 shows immunostaining for Ki-67, a cell proliferative marker. Fewer Ki-67-positive cells are observed in the miR-145 group, indicating a phenotype change in the VSMCs from the immature proliferative state to the mature contractile state.
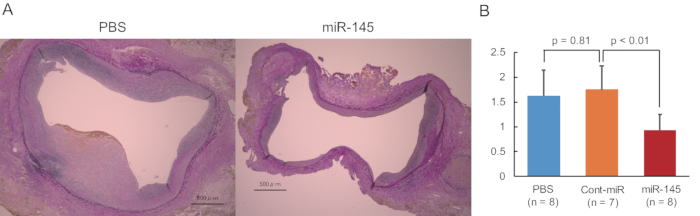
Figure 1: Successful intimal hyperplasia of the veins. (A) Representative Elastica Van Gieson staining for samples treated with PBS (upper panel) and with microRNA-145-loaded poly(lactic-co-glycolic acid) nanoparticles (lower panel). Scale bars = 500 µm. (B) Intimal area in the control PBS group, control microRNA group (Cont-miR), and microRNA-145 (miR-145) groups. MicroRNAs are loaded with poly(lactic-co-glycolic acid) nanoparticles. Statistical analyses were performed using one-way analysis of variance. Please click here to view a larger version of this figure.
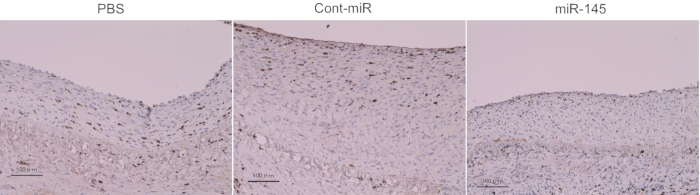
Figure 2: Cell proliferation. Ki-67 staining (brown). Scale bars = 100 µm. Please click here to view a larger version of this figure.
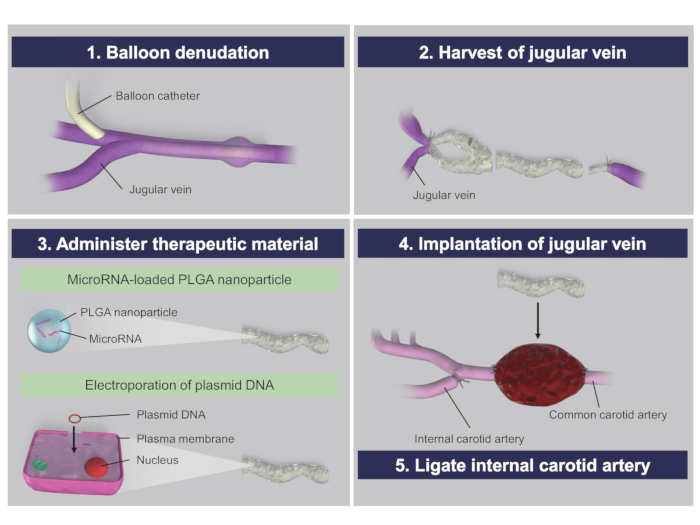
Figure 3: Procedural schema. DNA = deoxyribonucleic acid; PLGA = poly(lactic-co-glycolic acid); RNA = ribonucleic acid. Please click here to view a larger version of this figure.
Discussion
The present protocol is designed to provide an experimental platform to test various molecular or genetic interventions for VSMCs to control the phenotype from the proliferative to the contractile state and subsequently attenuate the progression of venous intimal hyperplasia in vivo. Using this model, we successfully prepared intimal hyperplasia at 2 weeks after surgery (Figure 1A) and indicated the therapeutic potential of microRNA-145 to control the VSMC phenotype26,27, validating the present protocol as a model to further investigate the attenuation of intimal venous hyperplasia.
Our rabbit intimal hyperplasia model consists of the following three major steps: 1) catheter injury; 2) jugular vein interposition; and 3) distal branch ligation (Figure 3). Vein grafts injured with a balloon catheter passage were shown to be deendothelialized, and the intima was proved to be hyperplastic23,28. In this protocol, we consider the catheter-injured vein grafts as saphenous vein grafts that are often manually pressurized and dilated in clinical settings for procedures such as coronary or peripheral artery bypass graftings. Moreover, distal branch ligation promoted intimal hyperplasia due to the reduced flow rate25. In the reported low-flow model, where the internal carotid artery and all the external carotid arteries except the most inferior branch were ligated, the neointima was more enhanced compared to that in the high-flow model with no distal branch ligation. In contrast, the distal branch ligation in this protocol did not include external carotid artery ligation to simplify and minimize the procedures, and the additional external carotid artery ligation in the present protocol may result in greater neointimal progression.
Existing rabbit intimal hyperplasia models have been developed to pursue either reproducibility or clinical validity. The initial model comprised only jugular vein interposition21. Afterwards a few modifications were made, including catheter injury or distal branch ligation, to augment the extent of the intimal hyperplasia23,25. In contrast, we aimed to establish a reproducible model resembling a clinical case, where patients with diabetes mellitus or peripheral artery disease often present poor distal perfusion on the coronary or lower extremity circulation. Moreover, saphenous vein grafts are often manually distended through hydrostatic pressure that causes endothelial exfoliation29. Considering these multiple factors inducing intimal hyperplasia, we adopted the mixed venous interposition model combined with the two additional procedures, mimicking a revascularization surgery.
This procedure requires surgical dissections on relatively superficial layers of the body, and the surgical incision is limited to the cervical region, making it less invasive for animals, resulting in a higher survival rate, and facilitating long-term observation. The surgical anastomoses are performed at the surface level of the body. This enables different researchers, not only surgeons, to conduct the procedure. The only critical step would be the anastomosis procedure mentioned in step 4.4. Inaccurate stiches may result in a stenosis or occlusion at the anastomosis site. When 8-0 polypropylene sutures are created, use of surgical telescopes with a magnification of at least 2.5x are recommended. As described in another report that addressed the rabbit intimal hyperplasia model26, 10-0 sutures with the aid of 10x power microscopes would also be helpful. After perfecting our model, our patency rate of the implanted vein graft at 2 weeks postoperatively was 90.9%. Another advantage of our model is the relatively lower procedure cost compared to that of large animal experiments. This enables investigators to increase the experimental volume to perform a larger number of interventions.
This venous interposition model is more clinically relevant, easy to handle, and low-cost. It can be applied to larger animal models and used for clinical studies. Although porcine and canine CABG models have been developed30,31,32, they are technically demanding. A porcine jugular vein interpose model that consists of jugular vein interposition alone has been established33. Thus, it is possible that the two procedures of catheter injury and distal branch ligation would be additionally performed as being more valid.
Another possibility is applying our model to a mouse venous interposition model. A reported mouse venous interposition model adopted a technically demanding cuff technique to circumvent direct anastomosis34. In the field of vein graft disease, mouse experimental models as well as larger animal models have been commonly used35. These include intimal hyperplasia models and vein graft atheroma models36. Techniques involved in the preparation for intimal hyperplasia models in mice include carotid artery ligation37, wire injury38, vein interposition, and collar injury39. In the vein graft atheroma models, genetically modified mice are typically used in mouse experimental models, in contrast to larger animal models. A mixed venous interposition model with the carotid artery ligation in genetically modified mice would be more clinically relevant.
A limitation of the present procedure is that the flow pattern at the site of the interposed vein is not the same as those of the vein grafts in human surgeries. In particular, the blood flow of the vein grafts on CABG is provided in the diastolic phase, wherein the flow pattern is different from that in the systolic phase. Another limitation is that the establishment of animal models recapitulating the etiology of the ischemia mediated by atherosclerosis in humans is challenging. The use of genetically modified animals with impaired lipid metabolism or on a high-fat diet may help overcome this limitation in the future.
Disclosures
The authors have nothing to disclose.
Acknowledgements
This work was supported by research grants from the Ministry of Education, Culture, Sports, Science and Technology, Japan (25462136).
Materials
| 10% Povidone-iodine solution | Nakakita | 872612 | Surgical expendables |
| 2-0 VICRYL Plus | Johnson and Johnson | VCP316H | Surgical expendables |
| 4-0 Silk suture | Alfresa pharma | GA04SB | Surgical expendables |
| 8-0 polypropylene suture | Ethicon | 8741H | Surgical expendables |
| Cefazorin sodium | Nichi-Iko Pharmaceutical | 6132401D3196 | Antibiotics |
| Fogarty Catheter (2Fr) | Edwards Lifesciences LLC | E-060-2F | Surgical expendables |
| Heparin | Nipro | 873334 | Anticoagulant |
| Intravenous catheter (20G) | Terumo | SR-OT2051C | Surgical expendables |
| Isoflurane | Fujifilm | 095-06573 | Anesthesia |
| Lidocaine hydrochloride | MP Biomedicals | 193917 | Anesthesia |
| Pentobarbital sodium | Tokyo Chemical Industry | P0776 | Anesthesia |
References
- Causes of death, 2000-2016, Global Health Estimates (GHE). World Health Organization (WHO) Available from: https://www.who.int/healthinfo/global_burden_disease/estimates/en/ (2019)
- Benjamin, E. J., et al. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association. Circulation. 139 (10), 56 (2019).
- Norgren, L., et al. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). Journal of Vascular Surgery. 45, 5-67 (2007).
- Caliskan, E., et al. Saphenous vein grafts in contemporary coronary artery bypass graft surgery. Nature Reviews: Cardiology. , (2020).
- Goldman, S., et al. Long-term patency of saphenous vein and left internal mammary artery grafts after coronary artery bypass surgery: results from a Department of Veterans Affairs Cooperative Study. Journal of the American College of Cardiology. 44 (11), 2149-2156 (2004).
- Muto, A., Model, L., Ziegler, K., Eghbalieh, S. D., Dardik, A. Mechanisms of vein graft adaptation to the arterial circulation: insights into the neointimal algorithm and management strategies. Circulation Journal. 74 (8), 1501-1512 (2010).
- Motwani, J. G., Topol, E. J. Aortocoronary saphenous vein graft disease: pathogenesis, predisposition, and prevention. Circulation. 97 (9), 916-931 (1998).
- Schachner, T. Pharmacologic inhibition of vein graft neointimal hyperplasia. Journal of Thoracic and Cardiovascular Surgery. 131 (5), 1065-1072 (2006).
- Kulik, A., et al. Secondary prevention after coronary artery graft surgery: a scientific statement from the American Heart Association. Circulation. 131 (10), 927-964 (2015).
- Gerhard-Herman, M. D., et al. 2016 AHA/ACC Guideline on the Management of Patients With Lower Extremity Peripheral Artery Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 135 (12), 686-725 (2017).
- Aboyans, V., et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries Endorsed by: the European Stroke Organization (ESO) The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). European Heart Journal. 39 (9), 763-816 (2018).
- Neumann, F. J., et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. European Heart Journal. 40 (2), 87-165 (2019).
- Alexander, J. H., et al. Efficacy and safety of edifoligide, an E2F transcription factor decoy, for prevention of vein graft failure following coronary artery bypass graft surgery: PREVENT IV: a randomized controlled trial. Journal of the American Medical Association. 294 (19), 2446-2454 (2005).
- Carrel, A., Guthrie, C. C. Uniterminal and biterminal venous transplantations. Surgery, Gynecology and Obstetrics. 2 (3), 266-286 (1906).
- Nabatoff, R. A., Touroff, A. S. The maximal-size vein graft feasible in the replacement of experimental aortic defects, long term observations concerning the function and ultimate fate of the graft. Bulletin of the New York Academy of Medicine. 28 (9), 616 (1952).
- Kanar, E. A., et al. Experimental vascular grafts. I. The effects of dicetyl phosphate on venous autografts implanted in the thoracic aorta of growing pigs: a preliminary report. Annals of Surgery. 138 (1), 73-81 (1953).
- Jones, T. I., Dale, W. A. Study of peripheral autogenous vein grafts. AMA Archives of Surgery. 76 (2), 294-306 (1958).
- Stehbens, W. E. Experimental production of aneurysms by microvascular surgery in rabbits. Vascular Surgery. 7 (3), 165-175 (1973).
- Bannister, C. M., Mundy, L. A., Mundy, J. E. Fate of small diameter cervical veins grafted into the common carotid arteries of growing rabbits. Journal of Neurosurgery. 46 (1), 72-77 (1977).
- Bergmann, M., Walther, N. Ultrastructural changes of venous autologous bypass grafts in rabbits: correlation of patency and development. Basic Research in Cardiology. 77 (6), 682-694 (1982).
- Murday, A. J., et al. Intimal hyperplasia in arterial autogenous vein grafts: a new animal model. Cardiovascular Research. 17 (8), 446-451 (1983).
- Quist, W. C., LoGerfo, F. W. Prevention of smooth muscle cell phenotypic modulation in vein grafts: a histomorphometric. Journal of Vascular Surgery. 16 (2), 225-231 (1992).
- Davies, M. G., Dalen, H., Svendsen, E., Hagan, P. O. Influence of perioperative catheter injury on the long-term vein graft function and morphology. Journal of Surgical Research. 66 (2), 109-114 (1996).
- Davies, M. G., Dalen, H., Svendsen, E., Hagan, P. O. Balloon catheter injury and vein graft morphology and function. Annals of Vascular Surgery. 10 (5), 429-442 (1996).
- Jiang, Z., et al. A novel vein grat model: adaptation to differential flow environments. American Journal of Physiology Heart and Circulatory Physiology. 286 (1), 240-245 (2004).
- Ohnaka, M., et al. Effect of microRNA-145 to prevent vein graft disease in rabbits by regulation of smooth muscle cell phenotype. Journal of Thoracic and Cardiovascular Surgery. 148 (2), 676-682 (2014).
- Nishio, H., et al. MicroRNA-145-loaded poly(lactic-co-glycolic acid) nanoparticles attenuate venous intimal hyperplasia in a rabbit model. Journal of Thoracic and Cardiovascular Surgery. 157 (6), 2242-2251 (2019).
- Ohno, N., et al. Accelerated reendothelialization with suppressed thrombogenic property and neointimal hyperplasia of rabbit jugular vein grafts by adenovirus-mediated gene transfer of C-type natriuretic peptide. Circulation. 105 (14), 1623-1626 (2002).
- Osgood, M. J., et al. Surgical vein graft preparation promotes cellular dysfunction, oxydative stress, and intimal hyperplasia in human saphenous vein. Journal of Vascular Surgery. 60 (1), 202-211 (2014).
- Shintani, T., et al. Intraoperative transfection of vein grafts with the NFkappaB decoy in a canine aortocoronary bypass model: a strategy to attenuate intimal hyperplasia. Annals of Thoracic Surgery. 74 (4), 1132-1137 (2002).
- Petrofski, J. A., et al. Gene delivery to aortocoronary saphenous vein grafts in a large animal model of intimal hyperplasia. Journal of Thoracic and Cardiovascular Surgery. 127 (1), 27-33 (2004).
- Steger, C. M., et al. Neointimal hyperplasia in a porcine model of vein graft disease: comparison between organ culture and coronary artery bypass grafting. European Surgery. 43 (3), 174-180 (2011).
- Thim, T., et al. Oversized vein grafts develop advanced atherosclerosis in hypercholesterolemic minipigs. BMC Cardiovascular Disorders. 12 (24), (2012).
- Zou, Y., et al. Mouse model of venous bypass graft arteriosclerosis. American Journal of Pathology. 153 (4), 1301-1310 (1998).
- de Vries, M. R., Simons, K. H., Jukema, J. W., Braun, J., Quax, P. H. Vein graft failure: from pathophysiology to clinical outcomes. Nature Reviews Cardiology. 13 (8), 451-470 (2016).
- Dietrich, H., et al. Rapid development of vein graft atheroma in ApoE-deficient mice. American Journal of Pathology. 157 (2), 659-669 (2000).
- Kumar, A., Lindner, V. Remodeling with neointima formation in the mouse carotid artery after cessation of blood flow. Arteriosclerosis, Thrombosis, and Vascular Biology. 17 (10), 2238-2244 (1997).
- Lindner, V., Fingerie, J., Reidy, M. A. Mouse model of arterial injury. Circulation Research. 73 (5), 792-796 (1993).
- Moroi, M., et al. Interaction of genetic deficiency of endothelial nitric oxide, gender, and pregnancy in vascular response to injury in mice. Journal of Clinical Investigation. 101 (6), 1225-1232 (1998).
