The present protocol was approved by and followed the Human Research and Ethics Committee guidelines of the National Institute of Medical Sciences and Nutrition Salvador Zubirán (Ref.: 1347). Informed consent was obtained from the human participants before participation in this study. Only patients in functional class I to III without total or partial arthroplasties18,19 and who were not candidates for prostheses were included in this study. Exclusion criteria included patients with cardiovascular disease, cancer, chronic kidney disease, pregnancy, or other autoimmune diseases that overlap with RA.
1. Recruitment of participants
- Recruit patients.
NOTE: For the present study, twelve women with RA were recruited from the rheumatology outpatient clinic. - Ensure that the patients receive stable pharmacological treatment during the previous 6 months; which could include any of the following: antimalarial drugs (e.g., chloroquine, hydroxychloroquine), disease-modifying antirheumatic drugs (DMARD) (e.g., methotrexate, leflunomide), and glucocorticoids (e. g., prednisone)20.
NOTE: According to the assessment by the rheumatologist, changes in pharmacological treatment could be made during the intervention period, if necessary.
2. Participant pre-test
NOTE: Pre-tests were performed 1 week before beginning the dynamic exercise program. Multifrequency bioelectrical impedance analysis equipment (see Table of Materials) was used, and measurements were performed with patients fasting for 4 to 5 h.
- Steps before testing
- Ensure that these measurements are carried out by a standardized person with extensive experience.
- Clean the equipment using 0.05% chlorhexidine and ensure that the hands are washed.
- Explain the procedure to the patient and obtain the measurements for the weight (kg) and height (cm).
- Ask the patient to remove both shoes and their right sock as well as any metal objects that are in contact with their skin.
- Place the patient in a supine position for 5 min with both legs and arms extended and verify that they are not in contact with any part of their body.
- Measurement of BIA
- Clean the back of the hand and the right foot with 70% alcohol.
- Place two electrodes on the back of the hand: one on the third metacarpophalangeal joint and the other in the middle of the wrist at the level of the head of the ulna.
- Place two electrodes on the right foot: one at the third metatarsophalangeal joint and the other between the medial and lateral malleoli. There should be a gap of 5-10 cm between the electrodes.
- Connect the four cables of the equipment. Once connected, place the red clamps on the electrodes close to the fingernail and toenail; place the black clamps on the remaining electrodes. The cables must not cross each other.
- The impedance values (Z) of four different frequencies (5, 50, 100, and 200 kHz) will be shown on the equipment screen. Note the resistance and reactance values for the 50 kHz frequency. These values will be necessary to classify patients with cachexia.
NOTE: Bioelectrical impedance analysis using tetrapolar multifrequency equipment provides accurate resistance and reactance values at a single frequency of 50 kHz as well as the ratio between the 200 kHz and 5 kHz impedance values (200/5 kHz).
- Classification of cachexia by BIVA
- Download the BIVA tolerance R-Xc graph software (see Table of Materials) and open it.
NOTE: The software is a spreadsheet that can be seen at the bottom of seven worksheets. - Go to the second worksheet, Reference populations; choose a row that corresponds to the reference population; copy it; and paste it in row two, marked in yellow.
NOTE: The reference population is chosen according to the age range, race, sex, and BMI of the population to be evaluated. - Go to the fifth worksheet, Fächer, and insert the patient's data in the second row: in column A, enter the patient's ID; in column B, enter the number one; and for the next two columns, one can choose whether to enter the patient's name.
- In column E, enter the patient's sex, using M for men or F for women. In columns F and G, insert the previously noted resistance and reactance values at 50 kHz. Enter the height (cm) and weight (kg) in the next two columns.
- In column J, enter the number corresponding to the reference population chosen in the second worksheet.
- Insert a number between 1 and 10 in column K. It will be needed for the "Point graph" sheet; in the next column, enter the patient's age.
NOTE: One can choose values between 1 and 10 because there can be up to 10 patients to graph simultaneously in the BIVA tolerance software. - The options bar is at the top of the software. Find the complements option and click it. Then, select the calculate option that will be displayed and click it. Observe the resistance and reactance values adjusted by height and phase angle.
- Next, navigate to sheet 3, Point Graph, and observe a BIVA graph according to the chosen reference population. A dialogue box will be displayed. Select the group code entered in column K for step 2.3.6. Select OK, and the BIVA graph will be shown with the patient's vector drawn as a geometric figure.
- Observe the tolerance ellipses of 50%, 75%, and 95% as well as the quadrants I, II, III, and IV in the BIVA graph. To classify a patient with cachexia using BIVA, the vector must be in the lower right quadrant (quadrant IV) and outside the 75% tolerance ellipse (Figure 1).
NOTE: Patients whose vectors fall in any of the quadrants within the <75% tolerance ellipses will be considered with a normal body composition classification21.
- Download the BIVA tolerance R-Xc graph software (see Table of Materials) and open it.
3. Dynamic exercise program
NOTE: The program was applied and supervised by a physiotherapist. An intervention duration of 48 sessions per patient was estimated. The exercise sessions were carried out in a mechanotherapy gym within a physiotherapy area belonging to the Rheumatology and Immunology department of the "INCMNSZ" with a duration of 90 min, twice a week.
- Evaluation of the session
- Ask patients about the pain or discomfort they perceive in their joints.
NOTE: The visual analogue scale (VAS) was used to assess pain. If they reported pain on the VAS above 7/10 in any joint, a more specific evaluation was carried out by the physiotherapy department (e.g., electrotherapy was used if there was only pain, thermotherapy was used if there was stiffness present, and cryotherapy was used when there was both pain and inflammation). - Take vital signs before each exercise session.
- Ask patients about the pain or discomfort they perceive in their joints.
- Warm-up
NOTE: With a duration of 15 min, a general dynamic warm-up divided into phases was established. Activation phase: simple, gentle, and global movements were performed for all movement arcs while remaining in a static position, with 10 to 15 repetitions. Set-up phase: in this last part, gentle dynamic exercises were performed, which simulated the gestures of the movements that would be implemented in the work phase, with 10-15 repetitions.- Activation phase
- Choose the most suitable warm-up exercise, including upper- and lower-extremity joints and their range of motion.
- Upper extremity: Instruct the patient to reach a range of motion with no discomfort for each joint movement. The instructor must lead the patient through a normal-speed movement and instruct the patient to avoid a painful range of motion.
- Lower extremity: Instruct the patient to perform the warm-up in a standing position with both feet on the ground and on a stable surface. Instruct the patient to reach a non-painful movement speed through the range of motion for each joint while the patient sits in a chair.
NOTE: If some patients can stand for a long time, a sitting position must be reached, considering a stable chair with the back straight and the feet on the ground. The available ranges of motion of the hip, knee, ankle, and feet must be included.
- Choose the most suitable warm-up exercise, including upper- and lower-extremity joints and their range of motion.
- Set-up phase
- Instruct the patient to perform functional movement patterns that include more than two joints per segment (lower limb or upper limb).
- Give supervision during this stage to bring a sense of wellness during the movement and adjust the range of motion when the patient presents discomfort.
- Activation phase
- Work phase
NOTE: With a duration of 60 min, the work phase is divided into three stages of 20 min each.- Aerobic: perform the work on a treadmill.
NOTE: Select a treadmill with no default inclination.- Ensure the emergency stop device is working correctly and explain the safety measures to the patient. Advise the patient to wear sports shoes.
- Give the patients information about the adaptations that must be performed when the treadmill starts and must be performed properly to avoid unnatural gait movements.
- Establish a base speed for each patient, asking for a normal feeling during walking.
- Adjust the speed after 5 min on the treadmill. Using a pulse oximeter (see Table of Materials), measure the heart rate while the speed is increased until reaching a heart rate zone between 55% and 75%14,31of the HRmax.
NOTE: If the patient's heart rate goes over the 75% HRmax, the speed must be reduced to the ideal heart rate zone. Instruct the patient to look for a comfortable pace. - After 10 min, ask the patient for an assessment using a perceived effort rating scale.
NOTE: The modified Borg rating of the perceived exertion scale was used to assess perceived exertion. - Lower the treadmill speed to a comfortable pace for the patient's last 5 min. The speed must be lowered to a total stop when reaching 5 min.
- Ask the patient for any pain or discomfort after the use of the treadmill.
- Resistance exercises
NOTE: Directed joint mobility exercises were used in combination with muscle strength exercises. The workout consisted of a set of 8-10 repetitions per exercise. Soft (0.5-2.6 kg) and medium (0.7-3.2 kg) resistance bands were used, and the resistance was gradually increased every 2 weeks. The dosage of the exercise depended on the state of the patient at the time of the intervention.- Upper Extremity
- Instruct the patient to perform upper-extremity mobility while handling a wooden stick (<1 kg) with both hands.
- Teach the patient combined exercises that include the range of motion of more than two joints (e.g., shoulder and elbow flexion).
- Instruct the patient to hold a band above the ends. The patient must roll up their hand with the end of the band to ensure their grip.
NOTE: If the patient's hands have discomfort, the instructor must gently secure the band to their wrist. - Instruct the patient to put one end of the band on the floor and step it with their foot. Then, perform elbow flexion against the band's resistance. Elbow extension must work on eccentric contraction while returning to the neutral position.
NOTE: The patient must be standing with a stable foot base and good posture. If the patient indicates some discomfort, this exercise must be performed in a sitting position. - Instruct the patient to roll up a band on their hand, ensuring no excessive pressure is applied. The other end should be held by the free hand of the patient next to the body at hip level. Then, instruct the patient to flex the elbow at 90° with the elbow in a neutral position.
NOTE: The patient can rest for 20 s between movements.
- Lower extremity
- Instruct the patient to sit in a stable chair with 90° hip and knee flexion and tie the ends of the resistance band, making a loop band. The patient must surround their legs with the rubber band at the distal part of the femur (above the knee). In this position, instruct the patient to perform hip flexions for each leg up to 20 to 30 degrees above the starting position.
NOTE: For correct alignment, avoid hip rotation and knee flexion. If the patient indicates discomfort, reduce the range of motion. - Instruct the patient to sit in a stable chair with 90° hip and knee flexion and tie the ends of the resistance band, making a loop band. The patient must surround their legs with the rubber band at the distal part of the femur (above the knee). In this position, instruct the patient to perform a slight hip flexion (above 10° from the base position) and hip abduction.
NOTE: For correct alignment, avoid hip rotation and excessive knee flexion. If the patient indicates discomfort, reduce the range of motion. - Instruct the patient to sit in a stable chair with 90° hip and knee flexion and tie the ends of the resistance band, making a loop band. The patient must surround the nearest chair leg and their own leg with the rubber band at the ankle. Instruct the patient to return, at a slow tempo, to the base position.
NOTE: For correct alignment, the patient must maintain a comfortable sitting position and avoid hip flexion compensation. If needed, the patient can hold the base of the chair with their hands for more stability. The steps can be performed with one leg at a time or by changing sides. - Instruct the patient to hold a standing position. Then, ask the patient to tie the ends of the resistance band, make a loop band, and place the band around their ankles. Instruct the patient to perform reps of changing positions between sitting and standing.
NOTE: If the patient feels discomfort during the exercise, reassess and make the exercise easy by using a higher chair to reduce knee flexion or using a second chair where the patient can support himself and facilitate movement.
- Instruct the patient to sit in a stable chair with 90° hip and knee flexion and tie the ends of the resistance band, making a loop band. The patient must surround their legs with the rubber band at the distal part of the femur (above the knee). In this position, instruct the patient to perform hip flexions for each leg up to 20 to 30 degrees above the starting position.
- Upper Extremity
- Recreation games
NOTE: Consisting of the implementation of exercise series that involve gestures or movements adapted from a particular sport such as soccer, basketball, or volleyball, integrating flexibility and coordination components, 4 to 7 stations consisting of polyarticular movements and different exercises are created, and two series of 8 to 15 repetitions are worked (with difficulty increasing every 2 weeks).- Choose the most suitable exercise based on a sporting gesture for the patients each session and make an exercise station. Each station must be designed taking into account the limitations of the patient.
- Make a soccer goal with two chairs with a 1.3 m separation between them.
- Instruct the patients to hit a 30 cm plastic ball with their feet at a 3 m spot in front of the soccer goal.
- Control the difficulty by increasing the repetitions or sets per station and by adding new stations to the circuit.
NOTE: Example station designs: (1) Attach a "Ula Ula" ring to the tip of a 1.3 m wooden stick, place the patient at a 2 m throwing point in front of the ring, and instruct them to throw a 30 cm plastic ball with their arms to the "Ula Ula ring". Each patient must score at least 5 times and can score up to 10 times. (2) Attach a rope along the room walls to simulate a volleyball net. The rope must have a minimum height of 1. 7 m, and two patients must be in position on each side. Instruct the patients to pass a 40 cm air balloon over the rope at least 10 to 15 times each. (3) Place two patients with a 3 m separation between them and instruct the patients to throw a 30 cm plastic ball with their arms. Each patient must throw the plastic ball at least 10 times per arm. Patients must always supervise.
- Aerobic: perform the work on a treadmill.
- Cooling
NOTE: Cooling has a duration of 15 min and is composed of active static stretches.- Applied globally, stretching must be performed gently without putting stress on the joint. Stretching should not produce discomfort for the patient.
- Maintain each stretch for 15 to 20 s.
4. Post-test evaluation
NOTE: The post-test assessment must be scheduled during the week after the last exercise session.
- Repeat the measurement of body composition to obtain the BIVA classification, as described in the pre-test.
NOTE: To make a comparison between before and after the implementation of the dynamic exercise program, it is necessary to obtain the mean of the resistance difference divided by the height (dR/H), the mean of the reactance difference divided by the height (dXc/H), and the standard deviation and the Pearson correlation coefficient of the differences with the following equation8:
- To obtain the change in the resistance and reactance, download the BIVA confidence software (see Table of Materials) and open it.
NOTE: The software is a spreadsheet; at the bottom, you can see five worksheets. - In the fourth worksheet, "Paired data", check for ten columns where it will be necessary to insert the requested data.
- In column A, place the group ID. In column B, place the number of patients that were evaluated.
- In column C, insert the mean of d R/H obtained previously. In the next column, add the standard deviation.
- In column E, insert the mean of d Xc/H, and in the following column insert the standard deviation. In column G, insert the correlation coefficient obtained previously.
NOTE: In column H, choose to place 1, where one can display the confidence ellipse on the chart, or option 2 if you want to show the confidence ellipse and the difference mean vector. - In the following two columns, one can choose whether to place the names of the group and the equipment that was used to make the measurements.
- Once all the necessary data are complete, go to sheet 5, "Paired graph". There, a graph of the means of the difference is visible, and will be able to locate the vector of the resistance and reactance mean, in addition to the confidence ellipse.
- To evaluate whether the change is statistically significant, locate the complements option in the toolbar and click it. It will open a box with Hotelling's T2 test statistic8, allowing one to locate the value of p.
Results are presented for six female patients with RA who participated in a 48 session dynamic exercise program. The mean age of the patients was 52.7 ± 13.1 years, and their BMI was 26.8 ± 4.6. The average disease duration was 15.5 ± 6.1 years, and the disease activity, measured by Disease Activity Score 28, was classified as low activity with an average of 1.9 ± 1. Regarding disability, the Health Assessment Questionnaire Disability yielded an average score of 0.5 ± 0.3. For the six participants who did not undergo the exercise program, the mean age was 55.8 ± 7, and their BMI was 27.2 ± 4.8. The disease duration was 21.8 ± 10, and the disease activity was similar to the group that underwent the dynamic exercise program.
Table 1 displays the pharmacological treatment of the groups, as well as the concentrations of C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR). No changes in pharmacological treatment were required for any patient during the intervention period, according to the treating rheumatologist.
Figure 2A illustrates the initial status of the six patients before the implementation of the dynamic exercise program. Each patient was positioned outside the 75% tolerance ellipses in the RXc graph, indicating cachexia according to the BIVA classification. The average resistance before the exercise program was 630 ± 88, and the reactance was 46.5 ± 7.4. Figure 2B demonstrates the change in BIVA classification after the implementation of the dynamic exercise program for the six patients shown in Figure 2A. They were reclassified as normal, according to BIVA. The average resistance was 577 ± 54.9, and the reactance was 57.5 ± 11.4.
Figure 3A shows the six patients who did not participate in the exercise program. Two patients were classified as cachexia, one as normal, and two as lean. Figure 3B displays the change in BIVA classification after 6 months for the patients shown in Figure 3A. According to the BIVA classification, the patients initially classified as lean moved to cachexia, and the patient initially in the normal classification also moved to cachexia.
The mean change in resistance per height (dR/H) after the implementation of the dynamic exercise program was -55.9 ± 51, and the mean change in reactance per height (dXc/H) was 10.7 ± 10.3. These changes are associated with increased cell membrane surface and membrane integrity (Xc component) relative to fluid volume (R component), reflecting higher body cell mass and improved cell function and muscle functionality (Figure 4A). In the group that did not undergo the dynamic exercise program, no statistically significant changes were observed after 6 months (Figure 4B).
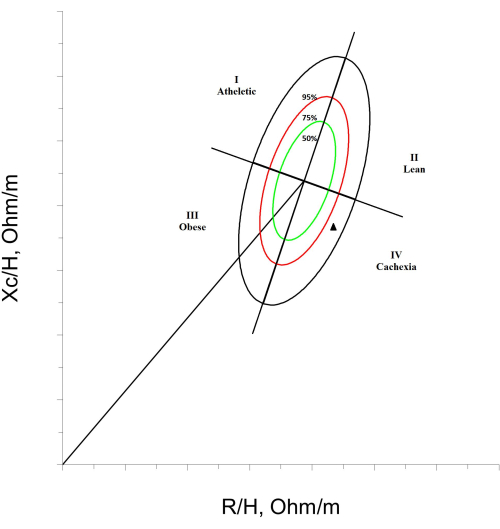
Figure 1: Cachexia classification by BIVA. An RXc graph is shown, divided into quadrants, with tolerance ellipses of 50%, 75%, and 95%. In the lower right corner, a patient with a cachexia BIVA classification, marked with a black triangle, is exemplified. Please click here to view a larger version of this figure.
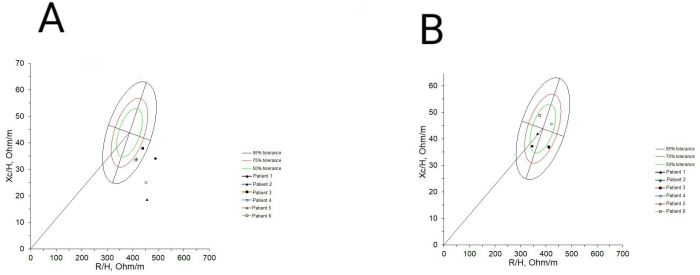
Figure 2: BIVA classification before and after implementing the dynamic exercise program. (A) The classification of the six patients before incorporating them into the exercise program is shown, and it can be observed that everyone had cachexia. (B) Changes in the BIVA classification after 48 sessions of the dynamic exercise program are shown, where it is observed that the six patients went from being classified with cachexia to being classified as normal. Please click here to view a larger version of this figure.
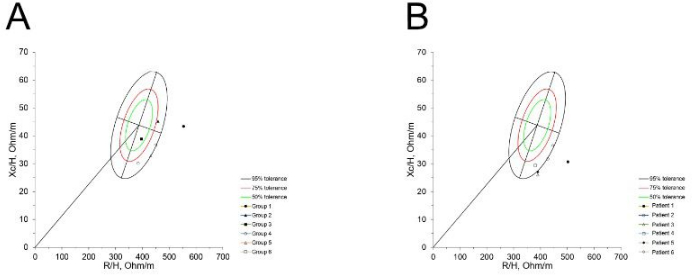
Figure 3: Basal BIVA classification and classification after six months in patients without an exercise program. (A) Classification of six patients at baseline measurement. (B) Changes after six months can be observed, where three patients shifted their classification to cachexia, while those who already had it remained unchanged. Please click here to view a larger version of this figure.
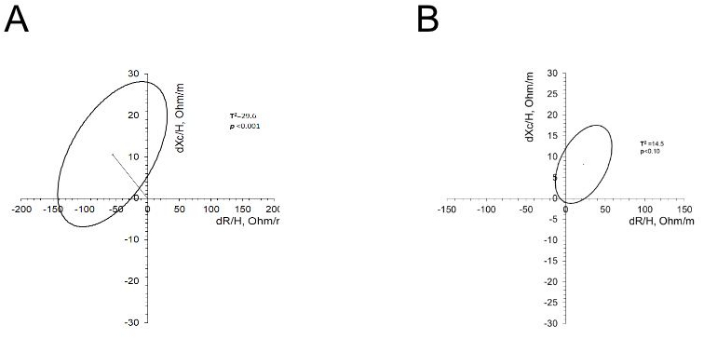
Figure 4: Changes in the R/H and Xc/H of patients who underwent an exercise program and those who did not. (A) The graph shows the vector of the mean of R/H and Xc/H and the confidence ellipse. The resistance decreased after the exercise program, while the reactance increased. (B) The graph shows the vector of the mean of R/H and Xc/H and the confidence ellipse. The resistance and reactance increased after six months. However, these changes were not statistically significant. Please click here to view a larger version of this figure.
| Variables | Dynamic exercise program | No dynamic exercise program |
| Age, years | 52.7 ± 13.1 | 55.8 ± 7 |
| Disease duration, years | 15.5 ± 6.1 | 21.8 ± 10 |
| Global Functional status, % | ||
| I | 33.3 | 33.3 |
| II | 66.6 | 33.3 |
| III | – | 33.3 |
| Disease activity score-28 | 1.9 ± 1 | 2.2 ± 0.8 |
| HAQ-Di, score | 0.5 ± 0.3 | 0.25 |
| BMI, kg/m2 | 26.8 ± 4.6 | 27.2 ± 4.8 |
| CRP, mg/dL | 1.2 ± 0.9 | 1.9 ± 1 |
| ESR, mm/h | 16.6 ± 8.5 | 12.5 ± 6.8 |
| Pharmacological treatment, % | ||
| Methotrexate | 100 | 83.3 |
| Sulfasalazine | 33.3 | 50 |
| Antimalarials | 66.6 | 16.6 |
| Leflunomide | – | 50 |
| Glucocorticoids | – | 33.3 |
| Glucocorticoid’s dose, mg | NA | 5 |
Table 1: Characteristics of the participants. The table displays the characteristics of six participants who underwent a dynamic exercise program for 48 sessions and six participants who did not undergo the exercise program. Data such as age, weight, disease duration, disease activity, disability, CRP and ESR concentrations, and prescribed pharmacological treatment are presented. Please click here to download this Table.
