- Sterile surgical instruments (Table 1) and 3″ cotton tipped applicators are placed on a sterile underpad. The bead sterilizer (Germinator 500) is turned on.
- Mice (age: > 6 weeks; wt: > 18g) are anesthetized with an i.p. injection of 20μl/g BW of tribromoethanol (250mg/kg; duration – approximately 40 minutes).
- When the mice are unresponsive to toe-pinch, a sterile lubricant (Tears Renewed) is applied to the eyes to protect them from desiccation and the left side of the chest is coated with depilatory (e.g. Nair) to remove fur from the skin.
- The depilatory is washed away with warm running water and betadine/alcohol swabbing is used to disinfect the surgical area.
- The mouse is placed on a warm deltaphase isothermal pad which is fixed to a plexiglass table. Each limb is immobilized using tape and a thick thread is placed horizontally under the top teeth to hold the upper jaw in place.
- The table is positioned vertically and a fiberoptic light is shone directly onto the neck region for transesophageal illumination. This requires precise placement such that the opening of the throat is viewed as a well lit orifice, thus enabling the trachea to be visualized to facilitate insertion of the PE tubing.
- The tubing is then connected to the ventilator (connected to a 95% O2/5% CO2) to administer constant positive pressure ventilation (TOPO ventilator; rate 125 breaths/min; peak inspiratory pressure 10-12 cmH2O; *note: settings vary with strain and gender 1-3). Once ventilation is confirmed by synchronous chest movements, the connection is fixed to the pad with tape to avoid extubation during the surgery.
- Using toothed forceps to pull skin up and away from the chest, a #10 sterile scalpel blade attached to a #3 scalpel handle is used to make a 1.5cm incision in the skin parallel to the sternum.
- Curved Vanna microscissors are used to cut the pectoralis muscles and make a small hole in the intercostal muscle.
- Straight, blunt microscissors are used to cut through 3 ribs.
- A 9mm pediatric ophthalmic speculum is used to retract the rib cage.
- Using the curved forceps, pull the pericardium away from the heart and use the toothed forceps to gently tear it open.
- Using the Castroviejo needle holder, a 6mm tapered point 3/8 needle threads the 8-0 polyethylene suture underneath the left anterior descending coronary artery (along the long axis of the heart) perpendicular to it.
- For a temporary ligature that can be removed for timed reperfusion, a sterile 0.5-1cm piece of PE90 is placed on the heart in parallel to the coronary artery. The suture, which has first been looped under the coronary artery, is then tied to the tubing. At the time it is to be released, the ligature is loosened. This can be repeated as desired and the time of occlusion/reocclusion can be modified 4. Depending on the length of the protocol and the type of anesthesia used, supplementation may be necessary.
- For a permanent occlusion, the ligature laced under the coronary artery is simply tied. Blanching and dyskinesia are apparent and the long end of the suture is cut 5-10.
- For intramyocardial injection(s), a sterile Hamilton syringe with a 30 gauge sterile beveled needle is introduced into the base of the heart above the area of injury on the right side of the ligature. The needle is then advanced into the area of injury and withdrawn slightly so that the bevel can be seen approximately at the border zone. Some of the solution in the syringe (2-3μl) is injected into the heart and the needle is held in place. The syringe is withdrawn another 1-3mm and the rest of the solution is injected. The syringe is held in place until the bleb that is formed by the solution dissipates. The needle is then removed. If there is any bleeding, a cotton-tipped applicator is gently pressed onto the needle insertion site until the bleeding stops 5-7.
- Once the myocardial manipulations are complete, the rib retractors are removed and the thoracic cavity is closed with 2-3 mattress sutures using 6-0 surgipro suture.
- Two-three mattress sutures are then made to close the pectoralis muscles, 1-3 drops of 0.25% marcaine 1:10 in sterile saline (0.1ml/25g mouse) is applied to the muscle and then 2-3 mattress sutures are made to close the skin.
- The mouse is removed from the ventilator. Once rhythmic, rapid, shallow breathing is verified, the mouse can be extubated.
- 0.5ml warm sterile saline is injected into the dorsal subcutaneous space and the mouse is placed on a warming pad in a cage until it regains mobility (1 hour minimum).
- For survival experiments, mice are placed back into their cages and returned to the vivarium until the time of sacrifice. During first 2 days, moistened food is placed on the cage floor to facilitate feeding (so they don’t have to reach up which may cause pain) and buprenorphine should be administered every 6-12hr. Post-operative care also includes daily monitoring for the first week to verify adequate mobility, grooming, and eating habits.
- The surgical instruments are wiped clean with ethanol and inserted into the bead sterilizer before the next surgery.
- At the time of sacrifice, mice are anesthetized with sodium pentobarbital (65mg/ml; 55-65 mg/kg). When an adequate plane of anesthesia is achieved, the thoracic cavity is opened.
- While the heart is still beating, a syringe with a 23 gauge needle containing cold potassium chloride (KCl, 30mM) or 2,3-butanedione monoxime (BDM; 10mM) is used to puncture the posterior basal region of the ventricle and the solution is slowly injected into the chamber until the heart is arrested in diastole.
- Once the heart is removed, a syringe containing PBS is used to retrogradely perfuse rinse the heart to remove any blood that remains. For acute studies, at the end of the reperfusion period, the LAD is re-ligated at the original point of occlusion. A solution containing 1% Evan’s blue is injected into the aorta. Once the heart is extracted, it is cut transversely into 3 sections of equal thickness, incubated in 1% 2,3,5-triphenyltetrazolium chloride, and imaged for morphometric analyses 11. For chronic studies, the heart is then immersed in fixative, then processed and embedded according to routine procedures. Slides can then be stained histologically and imaged for morphometric analyses (using Scion, NIH Image J, or Image Pro Plus) 9,10,12.
Representative Results:
When done correctly, the survival rates in mice (male: age 8-10 weeks, 22-28g; female: age 10-12 weeks, 20-26g) are: over 90% in acute ischemia/reperfusion and ischemic preconditioning experiments, over 85% in permanent artery ligation studies, and approximately 80% for intramyocardial injections. Since early injury is more readily visible by metabolic changes rather than structural, infarct size determination in ischemia/reperfusion and ischemic preconditioning experiments is performed by infusing 1% Evan’s blue dye into the aorta which will perfuse the heart that is not supplied by the LAD (Figure 1A). Once the heart is removed and transversely cut in half, the tissue is incubated in 1% solution of 2,3,5-triphenyltetrazolium chloride to measure infarct size (Figure 1B). The areas are measured using Scion or NIH imaging software which can be calibrated using a micrometer imaged at the same magnification. These numbers are used to calculate area at risk/left ventricle and infarct size/area at risk 11. Strain differences can result in variations in body weight and heart size and so care should be taken to normalize these measures to heart weight, body weight, or tibia length for comparative purposes.
Permanent artery ligation results in gross structural changes such as necrosis, wall thinning, and chamber dilation. Comparison of the effects of treatment and/or time on infarct size and necrosis relative to the left ventricle, chamber area, septal wall and left ventricular free wall thickness in the permanent occlusion model (Figure 2A) can also be measured using Scion or NIH imaging software. Collagen staining with picrosirius red/fast green (Figure 2B) can be used to measure insterstitial fibrosis which correlates to functional indices of wall stiffening8-10. The image in Figure 3 represents the distribution of 6ul solution (Evan’s blue) injected into the border zone of the heart following permanent artery ligation. Notice that it proceeds in the direction of the injury as well as toward the base and also transmurally.
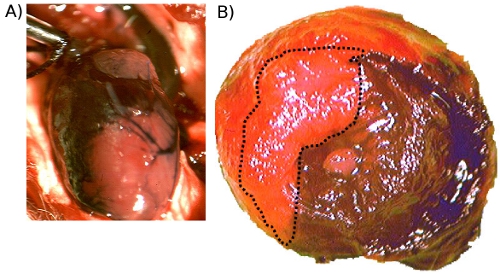
Figure 1. A. Evan’s Blue injected into the aorta prior to excision. This image shows the perfused regions of the heart (stained) and the occluded area (unstained). B. Evan’s Blue and TTC staining following acute ischemia/reperfusion injury. This is a representative image (20x) showing the blue dye distribution which stained the unoccluded regions as well as TTC staining of metabolically viable tissue (red). Necrotic areas do not stain and so they remain pale (outlined).
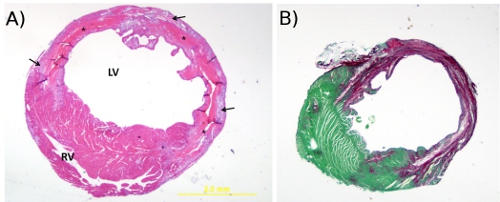
Figure 2. A. Hematoxylin and eosin stain. This is a representative image (20x) of H&E staining of a mouse heart cut transversely through the infarct region at 4 days post-MI (20x). The * denotes tissue necrosis, arrows point to granulation tissue, RV = right ventricle and LV = left ventricle. B. Picrosirius red and fast green stain. This is a representative image (20x) of picrosirius red/fast green staining of a cross-section of mouse heart at 4 weeks post-MI. The cytoplasm stains green and collagen fibers are red.
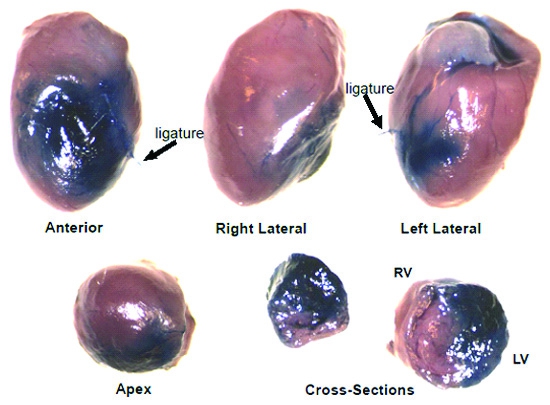
Figure 3. Evan’s Blue dye stain distribution following 6ul intramyocardial injection. This is a representative image showing the global and transmural distribution of Evan’s Blue dye throughout the heart following 6ul intramyocardial injection at the border zone immediately following coronary artery ligation (12x).
