In this study, the procedure was performed on 15 rats. At the end of 24 hours of saline infusion, no signs of saline or blood loss have been observed in the metabolic cages and the abdominal wound was clean in all animals as were the cages.
In the normal cages, rats were observed for 5 days with daily monitoring of weight and water/food intake. During this period, the general condition of the animals at gross examination was good with no indications of behavioral abnormalities. All rats immediately after surgery started feeding again. The average daily food and water intake increased progressively until normal after 3 days as shown in Figure 3A and 3B, respectively. In Figure 3C, it is possible to see that weight gain was regular, gradually increasing until the end of the observation period. No alterations of bowel movements took place and daily feces and urine output were normal.
After 24 hours, there was saline residue (respectively, 40 mL and 20 mL) in only 2 pumps filled with 50 mL of saline solution while all others (86.7%) were empty. Furthermore, after this infusion period, 12 cannulas (80%) were still functional for both blood sampling and saline infusion (5 mL), while 3 cannulas were not patent anymore (2 of these were the cannulas connected to the pumps with residue) (Table 1).
At necropsy, 100% of cannulas (n=15) were still located in the SMA branch and no rats had signs of bowel ischemia (Figure 4B) or intrabdominal bleeding. The 3 occluded cannulas were found kinked respectively at 0.5 cm, 1 cm and 1.5 cm from the insertion in the SMA branch. This phenomenon is probably due to the movements of the animals in the cages.
In 5 rats, immediately after the procedure and before pump connection, 2 mL of iodinated contrast medium were injected into the mesenteric cannula, to obtain an angiography through an image intensifier (angiography was performed intraoperatively). In each rat (n=5), it was possibile to see the mesenteric arterial circle and the SMA and its main branches without contrast medium spreading in the abdomen as shown in Figure 4A. This confirmed that the cannula was well placed and fixed to the branch of the SMA.
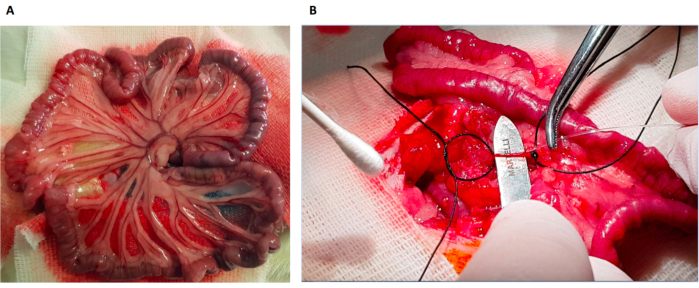
Figure 1: Experimental photographs. (A) The small intestine following its natural disposition on a gauze (it is possible to visualize the SMA with all the branches); (B) The operator inserting the cannula into the SMA branch. It is necessary to have a solid support under the vessel to guarantee the insertion of the tube. The distal silk suture closes the vessel and the proximal one fixes the catheter inside the branch. Please click here to view a larger version of this figure.
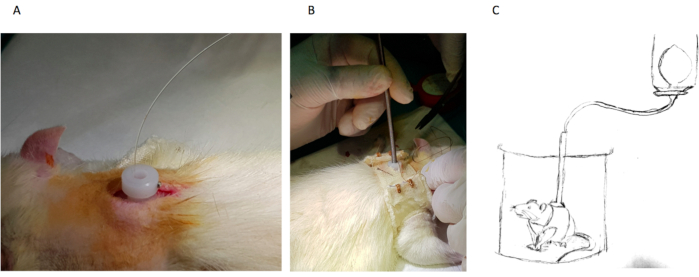
Figure 2: Infusion support system. (A) Once tunneled subcutaneously, the cannula emerges from the posterior region of the neck through the white valve; (B) A rat wearing a jacket to stabilize the white valve. A steel rod protects the catheter during infusion. (C) Diagramatic representation of a rat housed in a metabolic cage during infusion of saline with an elastomeric pump connected to the cannula exiting the steel rod. Please click here to view a larger version of this figure.
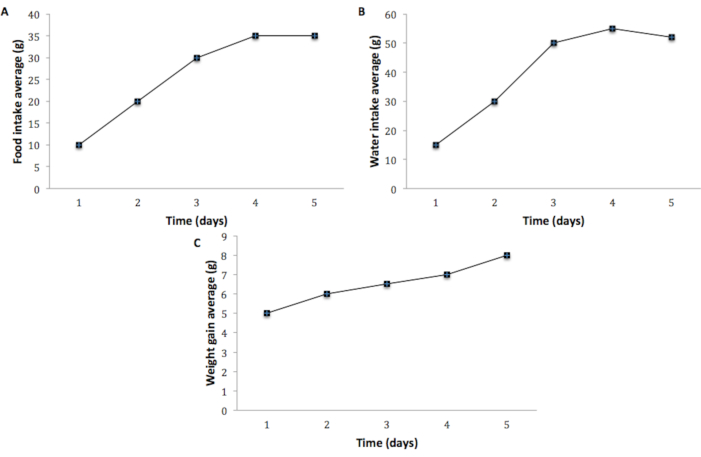
Figure 3: Representative data for food intake, water intake and weight gain of rats (n=15) in observation period of 5 days. The average daily food (A) and water (B) intake progressively increases, and it stabilizes at physiological levels after 3 days. The average weight gain (C) gradually increases until the end of the observation period. Please click here to view a larger version of this figure.
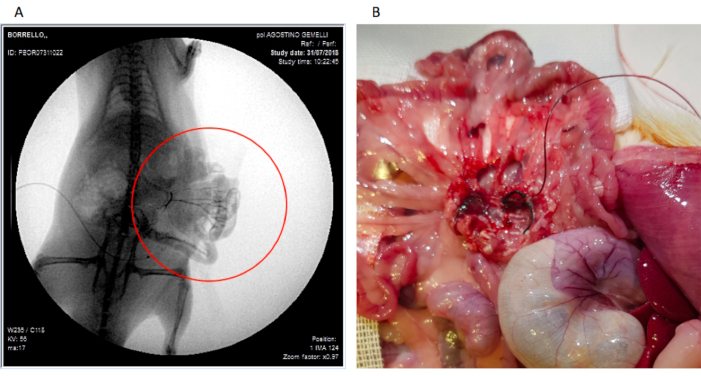
Figure 4: Photographs of (A) the contrast angiography of the mesenteric arterial region after contrast infusion through the cannula (proof of adequately placed cannula) and (B) the cannula still well positioned during autopsy. Please click here to view a larger version of this figure.
| Elastomeric pump | Cannula | |||
| Empty | With residue | Patent | Not Patent | |
| n=15 | 13 | 2 | 12 | 3 |
| % | 86.7 | 13.3 | 80 | 20 |
Table 1: Elastomeric pump dischargeand cannula patency after 24 hours of saline infusion. Patency was tested by drawing blood with a syringe and infusing 5 mL of saline in the cannula.
