The above protocol directs the isolation and staining of the TVA muscle for NMJ analysis. This allows whole-mount analysis of muscle innervation patterns as well as high-resolution analysis of NMJ morphology (Figure 2). This technique can be successfully applied to reveal NMJ pathology in mouse models of motor neuron disease, such as SMA4,17(Figure 3). In mouse models of SMA there is significant intramuscular variability in pathology, however the TVA muscle is consistently highly affected. This is evidenced by denervation of motor endplates, accumulation of neurofilaments at the presynaptic terminal and terminal sprouting (Figure 3). The results presented here thus demonstrate that the technique described above can be a powerful method to provide a comprehensive overview of innervation and analysis of NMJ pathology in mouse models.
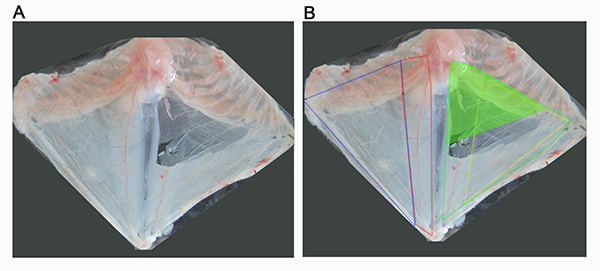
Figure 1. Overview of abdominal musculature of the mouse. (A) Image show the thoracic cage with attached abdominal musculature, which has been removed from a recently euthanized mouse and pinned out in a dissection dish superficial side up (A). (B) Dissection in A has been annotated to mark the approximate boundaries of the abdominal muscles. The superficial abdominal muscles can be seen on the left side of the dissection, and include external oblique (outlined in blue) and rectus abdominis (outlined in red). On the right hand side of the dissection, the superficial muscles have been removed allowed visualization of the transversus abdominis muscle (outlined in green) and the internal oblique muscle (outlined in yellow). The aim of this protocol is to direct the dissection of the superior part of the TVA muscle, shown here as a solid green triangle. Click here to view larger image.
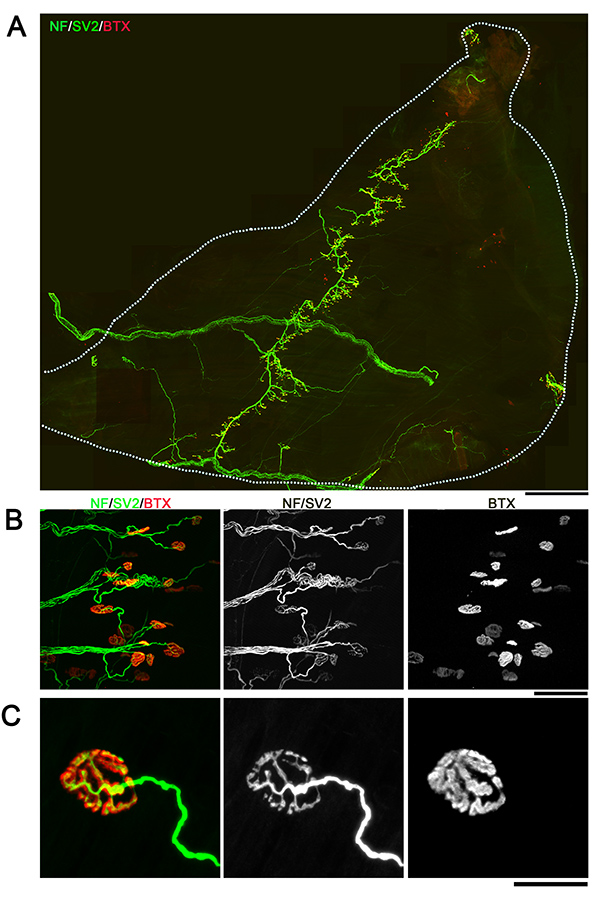
Figure 2. Whole-mount overview of neuromuscular junctions in TVA muscle. Images showing example NMJs from the TVA muscle visualized with immunofluorescent staining for neurofilament (NF; green), synaptic vesicle protein 2 (SV2; green) and bungarotoxin (BTX; red). Images are montaged fluorescent micrographs showing the whole muscle (A) or confocal images showing groups (B) or individual (C) NMJs. Scale bar = 800 µm (A), 70 µm (B), 25 µm (C). Click here to view larger image.
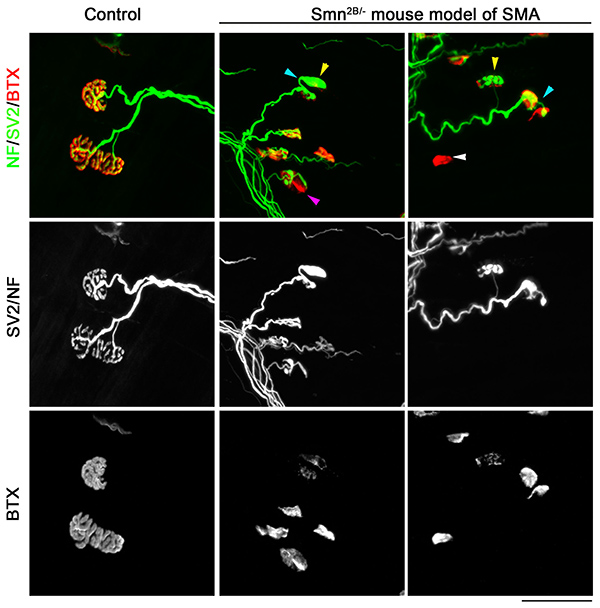
Figure 3. Neuromuscular junction pathology in TVA muscle from a mouse model of SMA. Confocal micrographs showing NMJs from the TVA muscle visualized with immunofluorescent staining for neurofilament (NF; green), synaptic vesicle protein 2 (SV2; green) and bungarotoxin (BTX; red) from either control (Smn2B/+) or SMA mouse model (Smn2B/-). Note that whilst normal NMJ morphology can be observed in control mice, in TVA muscles from Smn2B/- mice there is evidence of full denervation (white arrowhead), partial denervation (purple arrowhead) terminal sprouting (blue arrowhead) and presynaptic swelling (yellow arrowhead). The post-synaptic endplates are also less complex reflecting an apparently less mature phenotype. Scale bar = 50 µm. Click here to view larger image.
