Examples of flow cytometry analysis on gingival cells are presented. Gingival cells pooled from 2 mice were run in an LSR II flow cytometer and analyzed using FlowJo software. Figure 3A demonstrated the distribution of gingival cells from naïve mice in a side scatter (SSC) versus forward scatter (FSC) plot. Gating strategy to identify (i) lymphocytes (ii) monocytes / dendritic cells and (iii) granulocytes is indicated. For comparison purpose, we also present a FACS plot illustrating gingival cells purified from P. gingivalis infected mice 21 days after oral gavage in a setting of experimental periodontitis as we previously described (Figure 3B). An increase in the various immune cell populations can be easily detected in the infected mice as compared to naïve mice. Next, we identify immune cells in the processed gingiva by gating on cells expressing the hematopoietic marker CD45 (Figure 4A). These cells further segregated into CD3-positive cells representing T cells (Figure 4B). We also identified gingival neutrophils according to expression of the Ly6G and CD11b molecules (Figure 4C). Finally, langerhans cells, an epithelial subset of dendritic cells (DCs), were identified by gating on MHC class II+CD11c+ cells (a marker of murine DCs) and expression of Ep-CAM and langerin/CD207 (intracellular staining) (Figure 4D).
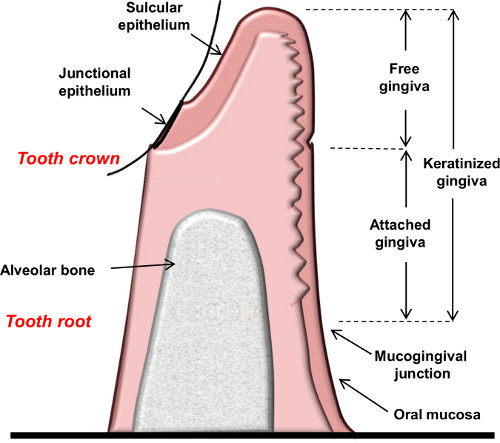
Figure 1. Schematic diagram showing the anatomical landmarks of the gingiva.
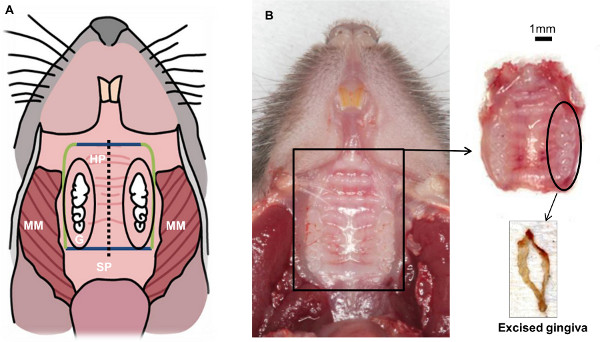
Figure 2. Schematic view of mouse oral cavity resulting after completing step 1.3. Soft tissues from the back to the front: masseter muscle (MM), soft palate (SP), hard palate (HP), gingiva (G). Hard tissue: molars and incisors. The main goal of this technique is to isolate the gingival tissue that surrounds the three molars (inside the black oval).
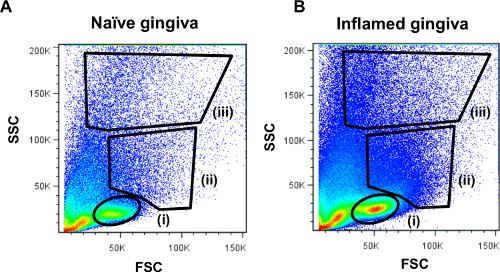
Figure 3. Representative FACS plots demonstrating cellular distribution of gingival leukocytes. Processed gingival samples were run on the LSR II flow cytometer and analyzed using FlowJo software. Side scatter (SSC) versus forward scatter (FSC) plots of the gingival cells from (A) naïve mice or (B) inflamed gingiva are presented. The location of (i) lymphocytes (ii) monocytes/dendritic cells and (iii) granulocytes populations is indicated.
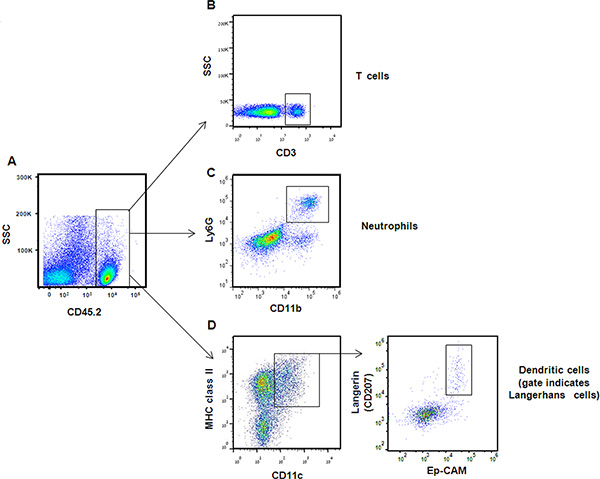
Figure 4. Representative FACS plots demonstrating analysis of immune gingival cells. (A) Immune cells were identified according to CD45 expression. Following gating on CD45-positive cells and lymphocytes population, expression of CD3 enabled targeting T-cell subset. (B) Neutrophils were identified in the gingiva according to ability of CD45+ cells to express also Ly6G and CD11b. (C) Dendritic cells were identified by gating on CD45+ cells from the monocyte/dendritic population [Figure 3, gate (ii)], and then on MHC class II and CD11c positive cells. (D) Langerhans cells were further segregated from other dendritic cells based on expression of Ep-CAM and the intracellular langerin molecule. Click here to view larger figure.
