When evaluating cell staining results for HEp-2, five major nuclear patterns are most commonly reported: homogenous, speckled, centromere, nucleolar, and nuclear dots. These patterns are the result of autoantibody binding to specific constituents of the nucleus. Although ANA testing is specific to nuclear structures, cytoplasmic patterns associated with autoantibodies against cytoplasmic structures may also be observed. In some cases, several autoantibodies may be present in a sample, and the image may appear as a mixed pattern.
There are other, less frequently observed, and often cell cycle specific patterns that can be detected by the IIF method; most recently, a so called dense fine speckled pattern with special clinical significance has been described in some ANA positive sera.
Homogeneous Pattern
To identify a homogeneous pattern, scan the well and identify mitotic or dividing cells. The condensed chromatin of the mitotic cells (Figure 2, orange arrow) exhibits solid, uniform fluorescence which is often more pronounced than in the resting cell nuclei.In the homogeneous pattern, the resting cells exhibit uniform, diffuse fluorescence of the entire nucleus (Figure 2, white arrow). This characteristic pattern is often the result of anti-dsDNA antibodies10.
Speckled Pattern
In the coarse speckled pattern, the mitotic cells show no staining of the condensed chromosomal regions (Figure 3, orange arrow). The resting cells exhibit granular fluorescence throughout the entire nucleus. The nuclear speckling can be defined as coarse or fine. The Coarse speckling pattern is often the result of anti-Sm and anti-RNP11.
In the fine speckled pattern, the resting cells show fine or diffuse speckling throughout the nuclei, typically in uniform distribution (Figure 4, white arrow). The fine speckled pattern is often the result of anti-SSAand anti-SSB12.
Dense Fine Speckled Pattern
It is now recognized that the dense fine speckled pattern (DFS) is common in routine testing, and as much as 12% of samples are positive for anti-DFS70 autoantibodies. However, these autoantibodies, when found in isolation, are not associated with systemic autoimmune rheumatic diseases4-6. These antibodies are prevalent in healthy individuals and patients bearing diseases unrelated to SARD6. Confirmatory testing for anti-DFS70 antibodies can help reduce unnecessary reflex testing, offer considerable cost savings, and ease patient anxiety.
Since the DFS pattern is difficult to identify and ANA positivity can cause anxiety to both patients and physicians, it is highly recommended to perform a confirmatory test after identifying a pattern suggestive of anti-DFS70 antibodies to clarify the clinical significance of ANA positivty5,6.
In this pattern, mitotic cells (Figure 5, orange arrow) show positive speckled staining of the metaphase chromatin, while resting cell nuclei (Figure 5, white arrow) exhibit uniformly distributed fine speckles throughout the nucleus.
Centromere Pattern
To identify the centromere pattern, scan the wells and identify mitotic or dividing cells. In mitotic cells (Figure 6, orange arrow), these discrete speckles become closely associated in what is often described as a “metaphase bar”. In the centromere pattern, resting cells (Figure 6, white arrow) show approximately 40-60 discrete speckles distributed throughout the nuclei. The centromere pattern is the result of anti-CENP A,B,C antibodies13.
Nucleolar Pattern
Some nucleolar patterns are associated with diffuse cytoplasmic staining in mitotic cells (Figure 7, orange arrow) and negative chromosomal region, while other nucleolear patterns display positive staining of the chromosomal region. The nucleolar pattern is associated with homogenous or speckled staining of the nucleoli (Figure 7, white arrow), along with weak speckled or homogenous staining of the nucleoplasm. These patterns are associated with anti-RNA polymerase III, anti-fibrillarin, anti-Th/To and anti-PM/Scl antibodies14,15.
Nuclear Dot Pattern
The nuclear dot pattern is associated with negative metaphase mitotic cells (Figure 8, orange arrow)and with few discrete speckles in the resting cell nuclei (Figure 8, white arrow). This characteristic pattern is often the result of sp-100, PML, or p80 colin autoantibodies. These antibodies are associated with primary biliary cirrhosis and autoimmune hepatitis16.
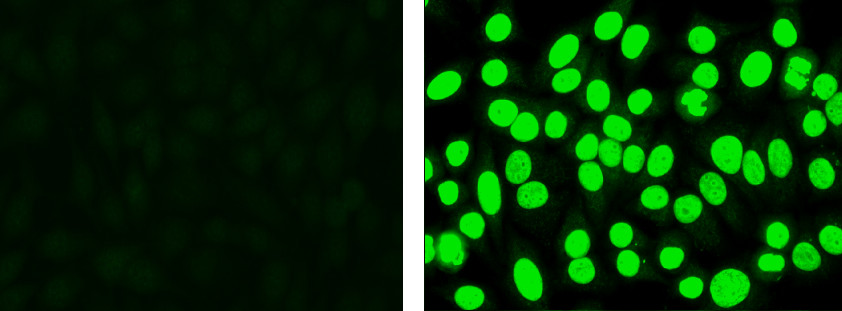
Figure 1. Negative control (left): Cells display low level non-specific fluorescence, but no specific nuclear staining. Positive control (right): Cells display apple green nuclear fluorescence.
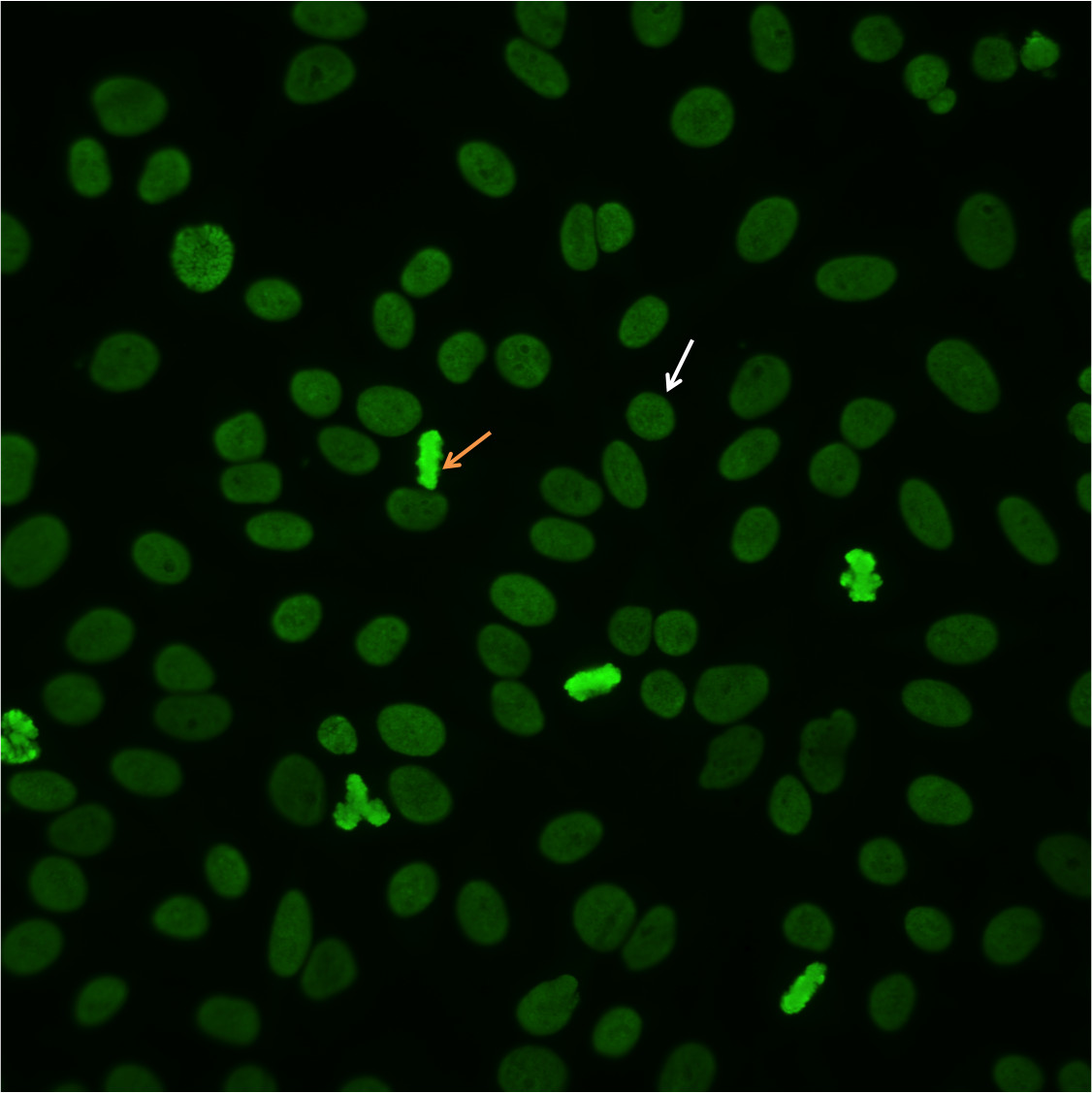
Figure 2. Homogenous pattern. Mitotic cells (orangearrow) show solid fluorescence. Resting cells show even, diffuse staining (whitearrow).
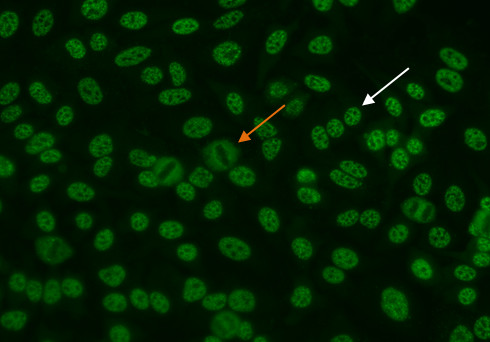
Figure 3. Coarse speckled pattern. Mitotic cells (orange arrow) show negative staining. Resting cells show a distinct speckled stain (white arrow).
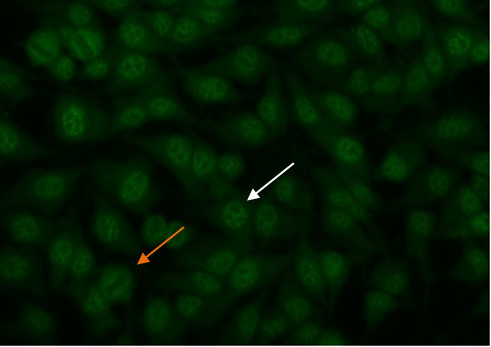
Figure 4. Fine speckled pattern. Mitotic cells (orange arrow) show negative staining. Resting cells show a distinct fine speckled staining (white arrow).
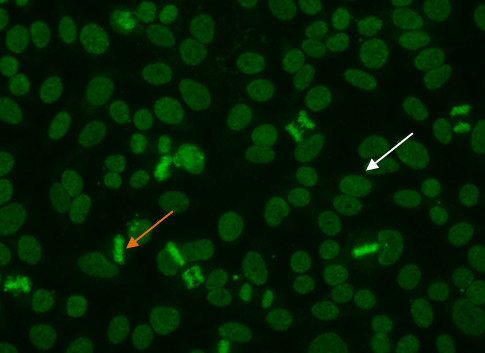
Figure 5. Dense fine speckled pattern. Mitotic cells (orange arrow) show a fine granular solid staining. Resting cells show a very fine, diffuse speckled stain (whitearrow).
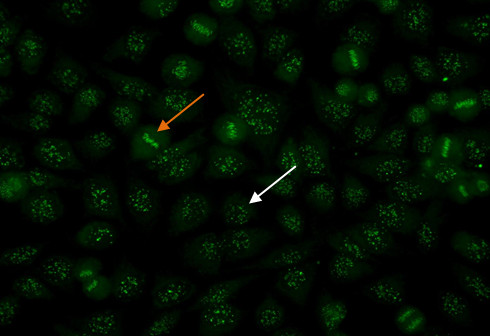
Figure 6. Centromere pattern. Mitotic cells (orangearrow) show uniform, discrete speckles. Resting cells (whitearrow) shows 40-60 discrete speckles per cell nucleus.
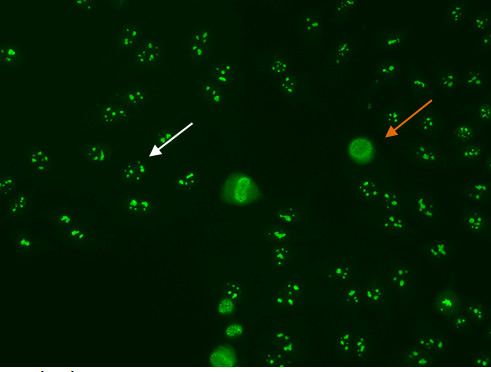
Figure 7. Nucleolar pattern. Mitotic cells (orangearrow) appear as large clusters of granular staining. Resting cell nucleishows fluorescence in the nucleoli(whitearrow).
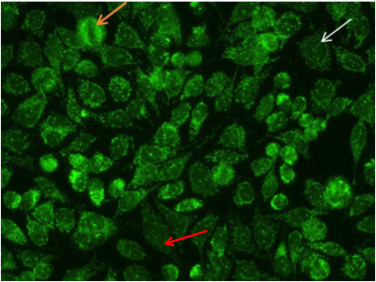
Figure 8. Nuclear dot pattern. Mitotic cells (orangearrow) appear negative. Resting cells show a few discrete speckles in the nucleus (whitearrow).Additionally, the nucelar dot pattern can coexist with cytoplasmic staining associated with autoantibodies to mitochondrial antigens (red arrow).
