The current method of organ preservation in liver transplantation is flush out with and subsequent storage of donor livers in cold (0-4 °C) preservation fluid (such as University of Wisconsin solution or Histidine-Tryptophan-Ketoglutarate solution). This method is referred to as static cold storage (SCS). Although the metabolic rate of livers at 0-4 °C is very low, there is still demand for 0.27 µmol oxygen/min/g liver tissue, which cannot be provided during SCS1. The conventional method of SCS, therefore, results in some degree of (additional) injury of donor livers. While this amount of preservation injury is not a problem in donor livers of good quality, it can become a critical and limiting factor in suboptimal livers that have already suffered some degree of injury in the donor. For this reason, livers with suboptimal quality or so-called extended criteria donor (ECD) livers are frequently rejected for transplantation as the risk of early graft failure is considered to be too high. High rates of delayed graft function, primary non-function, and non-anastomotic biliary strictures (NAS) have been described in recipients of livers from donation after circulatory death (DCD), older donors or recipients of steatotic grafts2. NAS are a major cause of morbidity and mortality after liver transplantation. NAS may occur in both extra- and intrahepatic donor bile ducts and can be accompanied by intraductal biliary sludge and cast formation3,4. Although the etiology of NAS is thought to be multifactorial, ischemia/reperfusion injury of the bile ducts during graft preservation and transplantation has been identified as a major underlying mechanism2,5. Transplantation of a DCD graft has been identified as one of the strongest risk factors for the development of NAS. The combination of a period of warm ischemia in a DCD donor, cold ischemia during organ preservation, and subsequent reperfusion injury in the recipient is thought to be responsible for irreversible injury of the bile ducts, which, in combination with a poor regenerative capacity of the bile ducts, results in fibrotic scarring and narrowing of the bile ducts after liver transplantation2,5. NAS have been reported in up to 30% of patients receiving a DCD liver6-8 . It has become clear that the current method of SCS of liver grafts for transplantation is insufficient for preinjured ECD livers such as those from DCD donors. Alternative methods are needed to increase and optimize the use of ECD livers for transplantation.
Machine perfusion (MP) is a method of organ preservation that may provide better preservation of donor organs, compared to SCS. MP could be especially relevant for the preservation of ECD grafts. An important advantage of MP is the possibility to provide oxygen to the graft during the preservation period. MP can be performed at various temperatures, which have been classified as hypothermic (0-10 °C), subnormothermic (10-36 °C) and normothermic (36-37 °C) MP (NMP). Depending on the temperature used for MP, the type of perfusion fluid has to be adjusted and with increasing temperature more oxygen should be supplied. The first clinical application of MP in human liver transplantation was based on hypothermic perfusion without active oxygenation of the perfusion fluid9,10. In animal models, hypothermic oxygenated MP (0-10 °C) has been shown to have protective effects against ischemia/reperfusion injury of liver grafts11 and to provide better preservation of the peribiliary vascular plexus of the bile ducts12. Subnormothermic oxygenated MP at 20 °C or 30 °C has also been studied in animal models and was shown to provide earlier recovery of graft function of DCD livers, compared to SCS13,14. The feasibility of subnormothermic oxygenated MP of human livers was recently reported in a series of seven discarded human donor livers15. NMP (37 °C) allows for the assessment of graft viability and functionality prior to transplantation16,17. Additionally, MP allows for gradual rewarming of the liver graft before transplantation, which has been demonstrated to facilitate recovery and resuscitation of the graft18.
The perfusion device used in the current protocol for hepatic machine perfusion enables dual perfusion (via the portal vein and the hepatic artery) using two centrifugal pumps, that provide a continuous portal flow and a pulsatile arterial flow. The system is pressure-controlled, allowing auto-regulation of the flow through the liver, depending on the intrahepatic resistance. Two hollow fiber membrane oxygenators allow for the oxygenation of the liver graft, as well as for the removal of CO2. The temperature can be set based on the intended type of MP (minimum temperature of 10 °C). Flow, pressure and temperature are displayed on the device in real-time allowing a continuous control of the perfusion process. A new sterile disposable set of tubing, reservoir and oxygenators is available for the perfusion of each graft (Figure 1).
The aim of this video article is to provide a step by step protocol for ex situ normothermic machine perfusion of human donor livers using this newly developed liver perfusion machine.
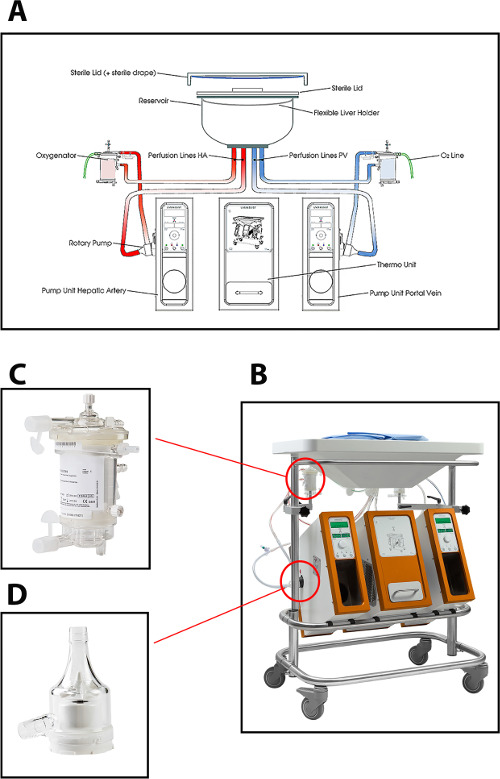
Figure 1: (A) A schematic drawing, (B) a photo of the perfusion machine, (C) a closer view of the oxygenator, and (D) centrifugal pump used for normothermic perfusion of human donor livers. Please click here to view a larger version of this figure.
