The protocol described permits the identification of surface and intracellular markers in T cells isolated from murine kidney, aorta and aortic draining lymph nodes in a model of angiotensin II induced hypertension. Representative results are presented below.
Figure 1 demonstrates the gating strategy used to identify the T cell population in a single cell suspension prepared from the aorta of a WT mouse infused with angiotensin II to induce hypertension. A similar strategy is used in the kidney and lymph nodes. The Forward Scatter Area (FSC-A) and Side Scatter Area (SSC-A) voltage was adjusted to detect the leukocyte population (G1) and to exclude debris. The live cells (G2) are negative for the viability marker conjugated with Pacific blue. Live cells were then gated on Forward Scatter Height (FSC-H) and Forward Scatter Area (FSC-A) to gate only on the singlet population (G3). Leukocytes were then selected by gating on SSC-A and CD45 (G4). CD45 is conjugated with AmCyan in this example. Finally, T cells are gated as the CD45+CD3+ population (G5). CD3 is conjugated with PerCP-Cy5.5 in this example.
To determine the presence of IL-17A and IL-17F producing T cells within murine kidney and aorta in this model, single cell suspensions were stained for IL-17A and IL-17F. Figure 2 illustrates fluorescence minus one controls (FMOs) for IL-17A and IL-17F staining in a kidney sample (conjugated with FITC and APC, respectively). FMO controls are samples that contain all the antibodies in a panel except for one. As expected, very few cells are positive for IL-17A (Figure 2A) or IL-17F (Figure 2B) in the FMO controls. These controls permit accurate discrimination of positive versus negative signals to properly adjust the gates to identify the cells positive for IL-17A or IL-17F in the experimental samples.
Figure 3 provides an example of intracellular staining of T cells isolated from kidney (Figure 3A) and aorta (Figure 3B) of WT mice infused with vehicle (Sham) or angiotensin II (Ang II). Indeed, a subset of T cells that express IL-17A or IL-17F can be detected in both tissues in this model.
Figure 4 illustrates intracellular staining of T cells within the aortic draining lymph nodes in this model (Figure 4A). CD8+ T cells were first gated (Figure 4B). Then, the expression of two Tc1 markers, the cytokine IFNγ or the transcription factor T-bet, were quantified from the CD8+ T cell subset. Figure 4C illustrates the FMOs for IFNγ and T-bet staining in the lymph node samples (conjugated with FITC and PE-Cy7, respectively). Figure 4D shows that in the aortic draining lymph nodes of WT mice infused with angiotensin II, a population of CD8+IFNγ+ and CD8+T-bet+ cells can be identified.
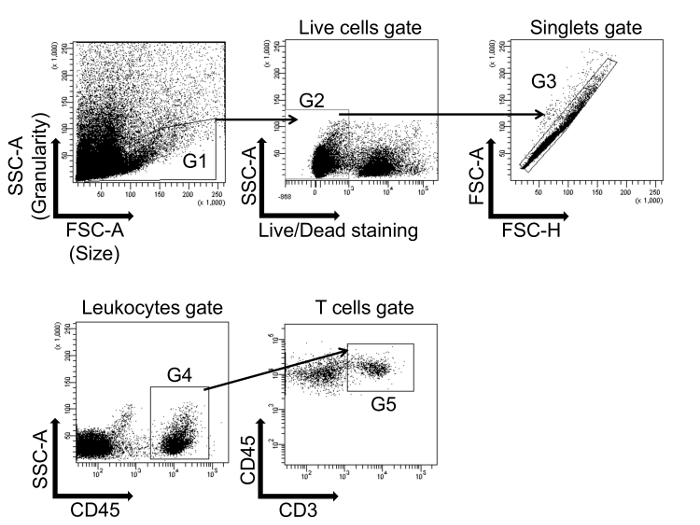
Figure 1: Flow cytometry gating strategy to identify T cells. Leukocytes are first gated on a forward scatter/side scatter (FSC-A/SSC-A) dot plot (G1), and live cells are selected (G2). The cells are then gated on singlets (FSC-A/FSC-H) (G3). Cells from G3 are further characterized by the expression of CD45 (G4). Finally, T cells are gated on CD45+CD3+ double positive cells (G5). This single cell suspension was prepared from the whole aorta isolated from a wild type (WT) mouse infused with angiotensin II to induce hypertension. Please click here to view a larger version of this figure.
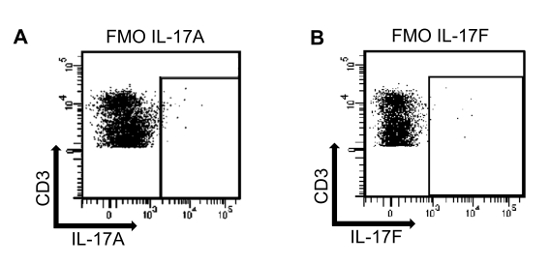
Figure 2: Fluorescence minus one controls (FMO) for IL-17A and IL-17F. (A) A single cell suspension isolated from an angiotensin II treated murine kidney sample was stained using a fixable viability marker (Pacific Blue), CD45 (AmCyan), CD3 (PerCP-Cy5.5) and IL-17F (APC). The antibody for IL-17A was omitted to determine the proper gating for IL-17A. (B) A single cell suspension isolated from an angiotensin II treated murine kidney sample was stained using a fixable viability marker (Pacific Blue), CD45 (AmCyan), CD3 (PerCP-Cy5.5) and IL-17A (FITC). In this case, the antibody for IL-17F was omitted. Please click here to view a larger version of this figure.
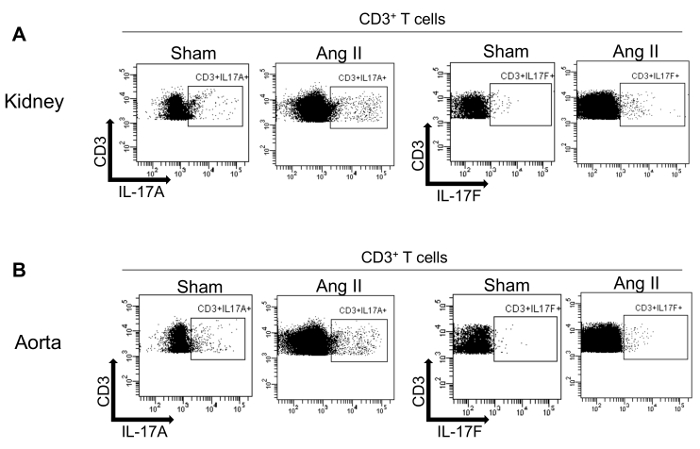
Figure 3: Intracellular staining of T cells isolated from murine kidney and aorta for IL-17A and IL-17F. Flow cytometry dot plots showing IL-17A and IL-17F expression in T cells from kidney (A) and aorta (B) from WT mice infused with vehicle (Sham) or angiotensin II (Ang II) and previously gated on CD45+CD3+ cells. Please click here to view a larger version of this figure.
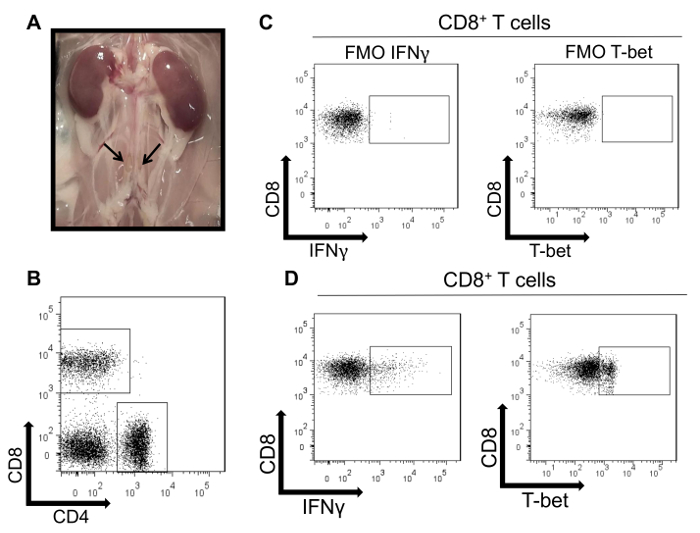
Figure 4: Intracellular staining of T cells isolated from murine aortic draining lymph nodes. (A) Macroscopic appearances of two lumbar aortic draining lymph nodes in a WT mouse. (B) Representative flow cytometry dot plots of CD4+ and CD8+ T cells isolated from four aortic draining lymph nodes isolated from a WT mouse infused with angiotensin II and previously gated on CD45+CD3+ cells. (C) A single cell suspension isolated from lymph nodes was stained using a viability marker (Pacific Blue), CD3 (PerCP-Cy5.5), CD4 (APC-Cy7), and CD8 (APC). FMO controls are shown in which the antibody for IFNγ (FITC) or T-bet (PE-Cy7) was omitted to determine the proper gating. (D) Flow cytometry dot plots demonstrating positive IFNγ and T-bet expression within CD8+ lymph node T cells using the gates determined by the FMO controls. Please click here to view a larger version of this figure.
