Retinal and RPE-choroid tissue can be processed in various ways to suit an individual investigation. After collection, the researcher will possess samples of retinal and RPE-choroid tissue from the foveal region, outer macula, and peripheral retina (Figure 1). Specifically, the foveal region punch will include the fovea, the parafovea, and a small amount of the adjacent perifovea. The macular punch includes the remainder of the perifoveal region as well as a small amount of the adjacent near-peripheral region. Finally, the peripheral punches sample the mid-peripheral and far-peripheral regions. In a representative experiment, tissue samples were trypsin-digested and analyzed using one-dimensional SDS-PAGE to visualize protein content (Figure 2A). The results of this analysis suggest distinct proteins among the different regions of the retina. Analysis by liquid chromatography-tandem mass spectrometry (LC-MS/MS)6 properly identified peptides from rhodopsin, a highly abundant and unique retina protein. A representative rhodopsin spectrum obtained from the macular region is shown in Figure 2B. Further analysis of the protein content will provide insights into the molecular functions of the anatomically distinct regions of the retina. In the case that the dissection is not performed carefully, and the retina is not properly separated from the RPE-choroid, differences in protein content between these two tissues will not be discernable.
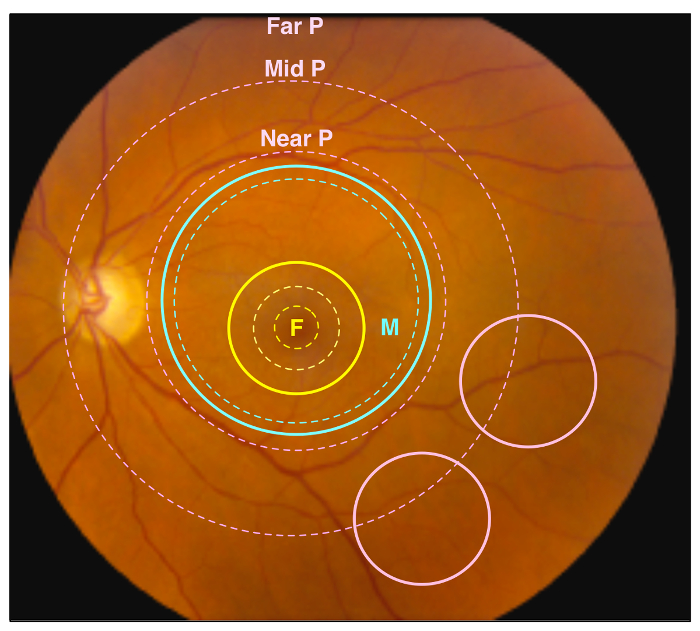
Figure 1. Retinal Regions. A representative image of a healthy human retina. Different retinal regions are highlighted by dotted circles, and regions sampled by punch biopsies are indicated by solid circles. The yellow dotted circles represent the foveal region, including the fovea, parafovea, and perifovea (traveling outward from center), while the yellow solid circle represents the 4 mm foveal punch. The blue dotted circle represents the anatomic macular region, while the blue solid circle represents the 8 mm macular punch. Finally, the pink dotted circles represent the near retinal peripheral region (Near P), mid retinal peripheral region (Mid P), and far peripheral region (Far P). The pink solid circles represent the 4 mm peripheral retina punches, which contain the Mid P and Far P regions. Please click here to view a larger version of this figure.
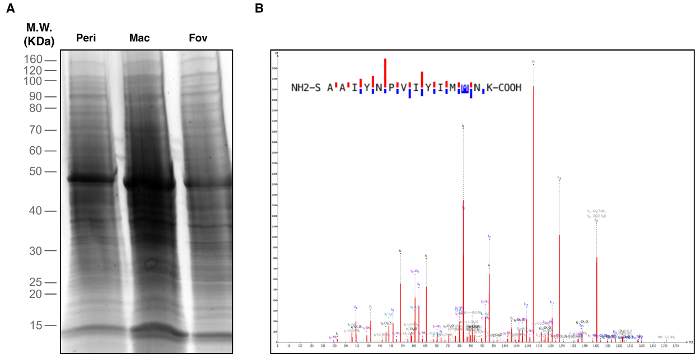
Figure 2. Identification of Retinal Proteins. Peripheral retina, macula, and foveal regions were biopsied and used for proteomic analysis. (A) One-Dimensional SDS-PAGE and silver staining visualized proteins in each retinal region. (B) Retina tissue samples were subject to liquid chromatography-tandem mass spectrometry (LC-MS/MS) analysis. The representative spectrum shown is of the rhodopsin protein identified in the macular region. This spectrum represents one of five unique rhodopsin peptides identified in the macula. Please click here to view a larger version of this figure.
