Der kardiogene Schock (CS) ist ein Zustand der Gewebehyperfusion mit oder ohne begleitende Hypotonie, bei dem das Herz nicht in der Lage ist, genügend Blut und Sauerstoff zu liefern, um den Bedarf des Körpers zu decken, was zu Organversagen führt. Es wird von der Society of Cardiovascular Angiography and Interventions (SCAI) in die Stadien A bis E eingeteilt: Stadium A – Patienten mit CS-Risiko; Stadium B – Patienten im Anfangsstadium von CS mit Hypotonie oder Tachykardie ohne Hypoperfusion; Stadium C – klassisches CS mit kaltem und nassem Phänotyp, der Inotrope / Vasopressoren oder mechanische Unterstützung zur Aufrechterhaltung der Perfusion erfordert; Stufe D – Verschlechterung der aktuellen medizinischen oder mechanischen Unterstützung, die eine Eskalation auf fortschrittlichere Geräte erfordert; und Stadium E – umfasst Patienten mit Kreislaufkollaps und refraktären Arrhythmien, die aktiv einen Herzstillstand mit laufender Herz-Lungen-Wiederbelebung erleiden1. Die häufigsten Ursachen für CS sind akute MI (AMI), die 81% der Fälle in einer kürzlich berichteten Analyse2 ausmachen, und akute dekompensierte Herzinsuffizienz (ADHF). CS ist klassisch durch Stauung und gestörte Perfusion gekennzeichnet, die sich in erhöhten Fülldrücken (pulmonaler kapillarer Keildruck [PCWP], linksventrikulärer enddiastolischer Druck [LVEDP], zentralvenöser Druck [CVP] und rechtsventrikulärer enddiastolischer Druck [RVEDP]), vermindertem Herzzeitvolumen (CO), Herzindex (CI), Herzleistung (CPO) und Fehlfunktion des Endorgans manifestieren3 . In der Vergangenheit waren die einzigen verfügbaren Behandlungen für AMI, die durch CS kompliziert wurden, die frühe Revaskularisation und die medizinische Behandlung mit Inotropen und / oder Vasopressoren4. In jüngerer Zeit, mit dem Aufkommen von Geräten zur mechanischen Kreislaufunterstützung (MCS) und der Erkenntnis, dass die Eskalation von Vasopressoren mit einer erhöhten Mortalität verbunden ist, gab es einen Paradigmenwechsel in der Behandlung von AMI und ADHF-bezogenem CS5,6.
In der heutigen Ära der perkutanen ventrikulären Unterstützungsgeräte (pVAD) gibt es eine Reihe von MCS-Geräteplattformen/-konfigurationen, die univentrikuläre oder biventrikuläre Kreislauf- und Ventrikelunterstützung mit und ohne Sauerstoffversorgungsfähigkeit bieten7. Trotz stetiger Zunahme der Verwendung von pVADs zur Behandlung von AMI und ADHF CS sind die Sterblichkeitsraten weitgehend unverändert geblieben5. Mit sich abzeichnenden Beweisen für mögliche klinische Vorteile bei der frühzeitigen Entladung des linken Ventrikels (LV) in AMI8 und der frühen Anwendung von MCS in AMI CS9 nimmt die Verwendung von MCS weiter zu.
Das MCS-Gerät (Left Atrial to Femoral Artery Bypass, LAFAB) umgeht die LV, indem es Blut aus dem linken Vorhof (LA) ablässt und über die Oberschenkelarterie in den systemischen arteriellen Kreislauf zurückführt (Abbildung 1). Es wird von einer externen Kreiselpumpe unterstützt, die je nach Größe der Kanülen einen Durchfluss von 2,5-5,0 Litern pro Minute (L / m) bietet (Pumpe der neuen Generation, die als LifeSPARC bezeichnet wird und einen Durchfluss von bis zu 8 l / m erreichen kann). Sobald das Blut über die transseptale Venenkanüle aus der LA extrahiert wurde, durchläuft es die externe Kreiselpumpe, die das Blut über die in der Oberschenkelarterie platzierte arterielle Kanüle in den Körper des Patienten zurückführt.
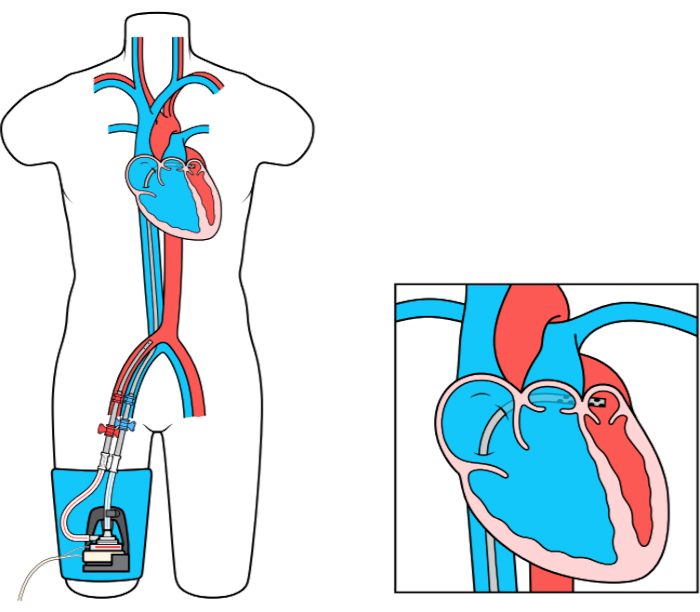
Abbildung 1: LAFAB-Setup. Mit freundlicher Genehmigung von TandemLife, einer hundertprozentigen Tochtergesellschaft von LivaNova US Inc. Bitte klicken Sie hier, um eine größere Version dieser Abbildung anzuzeigen.
