Intratibial Osteosarcoma Cell Injection to Generate Orthotopic Osteosarcoma and Lung Metastasis Mouse Models
Summary
The present protocol describes intratibia osteosarcoma cell injection to generate mouse models bearing orthotopic osteosarcoma and pulmonary metastasis lesions.
Abstract
Osteosarcoma is the most common primary bone cancer in children and adolescents, with lungs as the most common metastatic site. The five-year survival rate of osteosarcoma patients with pulmonary metastasis is less than 30%.Therefore, the utilization of mouse models mimicking the osteosarcoma development in humans is of great significance for understanding the fundamental mechanism of osteosarcoma carcinogenesis and pulmonary metastasis to develop novel therapeutics. Here, detailed procedures are reported to generate the primary osteosarcoma and pulmonary metastasis mouse models via intratibia injection of osteosarcoma cells. Combined with the bioluminescence or X-ray live imaging system, these living mouse models are utilized to monitor and quantify osteosarcoma growth and metastasis. To establish this model, a basement membrane matrix containing osteosarcoma cells was loaded in a micro-volume syringe and injected into one tibia of each athymic mouse after being anesthetized. The mice were sacrificed when the primary osteosarcoma reached the size limitation in the IACUC-approved protocol. The legs bearing osteosarcoma and the lungs with metastasis lesions were separated. These models are characterized by a short incubation period, rapid growth, severe lesions, and sensitivity in monitoring the development of primary and pulmonary metastatic lesions. Therefore, these are ideal models for exploring the functions and mechanisms of specific factors in osteosarcoma carcinogenesis and pulmonary metastasis, the tumor microenvironment, and evaluating the therapeutic efficacy in vivo.
Introduction
Osteosarcoma is the most common primary bone cancer in children and adolescents1,2, which mainly infiltrates the surrounding tissue, and even metastasizes to the lungs when the patients are diagnosed. Pulmonary metastasis is the main challenge for osteosarcoma therapy, and the five-year survival rate of osteosarcoma patients with pulmonary metastasis remains as low as 20%-30%3,4,5. However, the five-year survival rate of primary osteosarcoma has been increased to about 70% since the 1970s due to the introduction of chemotherapy6. Therefore, it's urgently needed to understand the fundamental mechanism of osteosarcoma carcinogenesis and pulmonary metastasis to develop novel therapies. The application of mouse models that best mimic the osteosarcoma progression in humans is of great significance7.
The osteosarcoma animal models are generated by spontaneous, induced genetic engineering, transplantation, and other techniques. The spontaneous osteosarcoma model is rarely used due to the long tumor formation time, inconsistent tumor occurrence rate, low morbidity, and poor stability8,9. Although the induced osteosarcoma model is more accessible to obtain than the spontaneous osteosarcoma, the application of the induced osteosarcoma model is limited because the inducing factor will affect the microenvironment, the pathogenesis, and pathological characteristics of osteosarcoma10. Transgenic models are helping to understand the pathogenesis of cancers since they can better simulate the human physiological and pathological environments; however, the transgenic animal models also have their limitations due to the difficulty, long-term, and high cost of transgenic modification. Moreover, even in the most widely accepted transgenic animal models generated by p53 and Rb gene modification, only 13.6% of sarcoma occurred in the four limb bones11,12.
Transplantation is one of the most commonly used primary and distant metastatic cancer model-producing methods in recent years due to its simple maneuver, stable tumor formation rate, and better homogeneity13. Transplantation includes heterotopic transplantation and orthotopic transplantation according to the transplantation sites. In osteosarcoma heterotopic transplantation, the osteosarcoma cells are injected outside the primary osteosarcoma sites (bone) of the animals, commonly under the skin, subcutaneously14. Although the heterotopic transplantation is straightforward without the necessity to perform surgery in animals, the sites where the osteosarcoma cells are injected do not represent the actual human osteosarcoma microenvironment. Osteosarcoma orthotopic transplantation is when the osteosarcoma cells are injected into animals' bones, such as tibia15,16. Compared to the heterotopic grafts, orthotopic osteosarcoma grafts are characterized by a short incubation period, rapid growth, and strong erosive nature; therefore, they are ideal animal models for osteosarcoma-related studies17.
The most commonly used animals are mice, dogs, and zebrafish18,19. The spontaneous model of osteosarcoma is usually used in canines because osteosarcoma is one of the most common tumors in canines. However, the application of this model is limited because of the long tumor formation time, the low tumorigenesis rate, poor homogeneity, and stability. Zebrafishes are often used to construct transgenic or knockout tumor models because of their rapid reproduction20. But zebrafish genes are different from human genes, so their applications are limited.
This work describes the detailed procedures, precautions, and representative images for producing the primary osteosarcoma in the tibia with pulmonary metastasis via intratibia injection of osteosarcoma cells in athymic mice. This method was applied to create the primary osteosarcoma in mouse tibia for therapeutic efficacy evaluation, which showed a high reproducibility21,22.
Protocol
All animal experiments were approved by the animal welfare committee of Shanghai University of Traditional Chinese Medicine. Four-week-old male BALB/c athymic mice were acclimated for a week before the surgery for orthotopic injection of osteosarcoma cells. Mice were housed in individually ventilated mice cages with five mice per cage in a 12-hour light/dark cycle with ad libitum access to SPF feed and sterile water.
1. Preparation of cells
- On the day of osteosarcoma cell (143B-Luciferase) injection, wash 80%-90% confluent cells cultured in a 10 cm cell culture dish twice with PBS (pH 7.4) and trypsinize with 1.5 mL of 0.25% trypsin for 3 min. Then, add 6 mL of 10% serum-containing MEM media to quench the trypsin, and collect the cells in a 15 mL centrifuge tube.
NOTE: 143B-Luciferase cell line is obtained from 143B cell line transfect with pLV-luciferase vector23. - Aspirate 20 µL of cell suspension into the chamber of cell counting plate and calculate cell concentration using an automatic cell counter (see Table of Materials).
- Centrifuge the cells at 800 x g for 5 min at room temperature.
- Aspirate the supernatant with a pipette and resuspend the cell pellet in an 8.5 mg/mL basement membrane matrix (see Table of Materials) to a final concentration of 2 x 107 cells/mL.
- Keeping the cells on ice, bring them to the surgery room. The cells are to be used within 2 h.
NOTE: To avoid inaccurate injection doses (for example, due to the dead space in syringes), an extra cell suspension is prepared (usually two times the required volume of cell suspension). The basement membrane matrix is kept on ice all the time since it has coagulation property above room temperature24.
2. Surgery for orthotopic injection of the osteosarcoma cells
NOTE: The surgery tools are shown in Figure 1.
- Mice were raised in specific pathogen-free conditions. All procedures were done in an aseptic cabinet with sterile tools.
- Anesthetize the mice by exposing them to 2% isoflurane and 98% oxygen (oxygen flow rate, 2 L/min).
- Apply a small amount of ophthalmic ointment on the eyes to prevent dryness while under anesthesia.
NOTE: Perform the entire procedure in a well-ventilated area. Before osteosarcoma cell injection, ensure that each mouse is under deep anesthesia by a toe pinch; if the mouse still has responses, such as twitch or jerk, wait for a long time until the above responses disappear. - Keep each mouse in a supine position. Hold the ankle of the mouse using the thumb and index finger and disinfect the injection site of the tibia with a 70% ethanol swab.
NOTE: To tightly hold the mouse ankle, both the thumb and index fingertips are of great importance for the subsequent procedures. - Rotate the ankle joint of each mouse outward to move the tibia and fibula, and bend the knee joint to a suitable position until the proximal tibia plateau (the top of the tibia) is clearly visible through the skin (Figure 2A).
- Attach the needle to a 1 mL syringe and point the needle tip toward the injection site. Ensure that the syringe needle is parallel to the long axis of the tibia.
- Percutaneously insert the needle through or adjacent to the patellar ligament as it goes through the skin/joint capsule; th0en, rotate the syringe (1/2 to 3/4-circle) to drill a hole through the tibia platform toward the distal end of the tibia (medullary cavity) for osteosarcoma cell injection with a micro-volume syringe (Figure 2B,C).
NOTE: Simultaneous rotation of the tibia can be felt while drilling if the needle tip is accurate. Ensure the needling moves forward with the syringe rotation rather than being directly pushed forward until about half of the needle is in the tibia.
- Percutaneously insert the needle through or adjacent to the patellar ligament as it goes through the skin/joint capsule; th0en, rotate the syringe (1/2 to 3/4-circle) to drill a hole through the tibia platform toward the distal end of the tibia (medullary cavity) for osteosarcoma cell injection with a micro-volume syringe (Figure 2B,C).
- Check whether the syringe needle made a prominent movement into the medullary canal to ensure successful drilling.
NOTE: Perform an X-ray examination (see Table of Materials) to confirm the proper position of the needle and collect the images. - Load 143B osteosarcoma cell suspension (from step 1.5) into a micro-volume syringe and replace the 1 mL syringe in the tibia with the 143B cell-loaded micro-volume syringe (Figure 2D). Slowly inject ~10 µL (ignore pre-existing solution in the needle) of 143B cell suspension into each athymic mouse's tibia (about 2 x 105 cells) without applying high pressure.
- Press the injection site with a cotton swab for 20-30 s when the micro-volume syringe is removed.
- Put each mouse back into a clean cage and closely monitor until the mouse is completely recovered from anesthesia (about 10 min).
- Monitor the tumor growth in vivo using an X-ray imaging system. Measure the longer diameter (a) and the short diameter (b) of the cancer mass every week with a caliper for tumor volume (V) calculation: V = 1/2 x a x b2.
NOTE: Anesthetize the mice by exposing them to 2% isoflurane and 98% oxygen. The mice were anesthetized for x-ray imaging. Intratibia injection of luciferase or fluorescent protein labeled osteosarcoma cells enables tracking of primary and metastatic osteosarcoma lesions.
NOTE: Humane endpoints of the mice with osteosarcoma due to tumor growth of the knee and lung metastasis were based on the following criteria: (1) Body Condition Score, (2) weight loss threshold of 20%, (3) average maximum diameter of tumors of 2 cm, or (4) severely limited animal behavior.
3. Pathologic examination (collecting primary and pulmonary metastatic osteosarcoma specimen for analysis)
- Six weeks after osteosarcoma cell injection, sacrifice the mice by cervical dislocation after exposing them for CO2 inhalation.
- Keep the mouse in a supine position and stretch both the hind limbs.
- Separate the whole legs bearing osteosarcoma from the inguinal area.
NOTE: Ensure that all legs are separated from the same anatomical site. - Prepare the histological specimen of legs bearing osteosarcoma by removing the skin, muscles, and feet, and then fix the specimen of each mouse in a 50 mL tube with 20 mL formalin solution (10%) for 24 h, followed by decalcification in 10% EDTA solution for 14 days with occasional buffer change.
- Embed the specimen in paraffin and prepare sections for histological examination following previously published work25.
- Gently separate the lungs and put them into a 50 mL tube filled with 20 mL formalin solution (10%). After 24 h, transfer the lungs of each mouse into a 15 mL tube with 70% ethanol. Embed the lungs in paraffin for Hematoxylin and Eosin (H&E) staining and immunohistochemistry assay25.
Representative Results
Successful orthotopic (primary) osteosarcoma and metastatic pulmonary models depend on the accurate orthotopic injection of osteosarcoma cells. Here, an orthotopic (primary) osteosarcoma model via intratibial osteosarcoma cell injection was successfully developed. Figure 3A shows a representative mouse bearing orthotopic (primary) osteosarcoma, and Figure 3B shows a representative isolated orthotopic (primary) osteosarcoma. The tumor volume was measured once a week with a caliper and calculated as described in step 2.11 (Figure 3C). The orthotopic (primary) osteosarcoma growth in vivo was tracked by both the X-ray and the bioluminescence (when the injected cells were labeled with luciferase) live imaging system. The X-ray images were obtained from the first week to the sixth week after 143B osteosarcoma cell injection (Figure 3D). Furthermore, the image of orthotopic (primary) osteosarcoma growth in vivo was obtained after luciferase labeled 143B cells were injected into the mouse tibia (Figure 3E).
The pulmonary metastasis caused by the intratibial injection of luciferase labeled osteosarcoma cells was successfully tracked in vivo by a bioluminescence live imaging system (Figure 4A). The metastatic colonies in the isolated lung tissues were also visualized under the stereomicroscope (Figure 4B). The metastatic lesions were further confirmed by H&E staining on paraffin-embedded lung tissues (Figure 4C).

Figure 1: Surgery Tools. (A) 1 mL scale syringe. (B) Micro-volume syringe. Please click here to view a larger version of this figure.
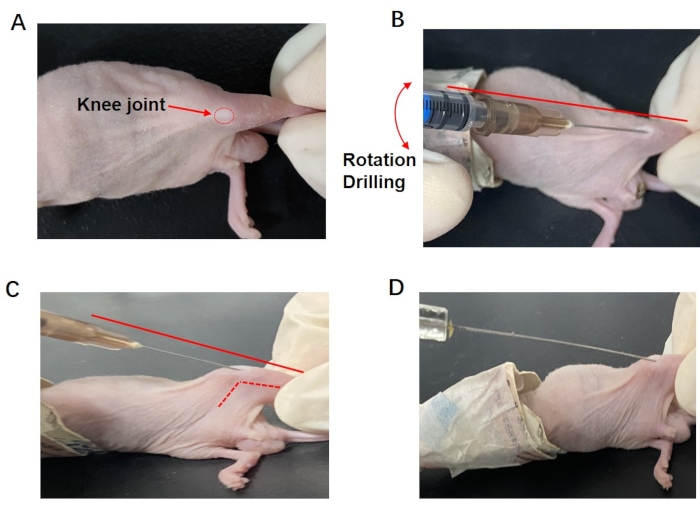
Figure 2: Representation of the intratibial injection surgery. (A) The intratibial injection site of an athymic mouse. (B) A sterile 1 mL syringe with an accompanied needle was percutaneously inserted into the tibia toward the distal end via the proximal tibia plateau (the top of the tibia). (C) A lateral view of the drilling process. The syringe needle was parallel to the long tibia axis (solid line). (D) Intratibial injection with osteosarcoma cell loaded micro-volume syringe. Please click here to view a larger version of this figure.
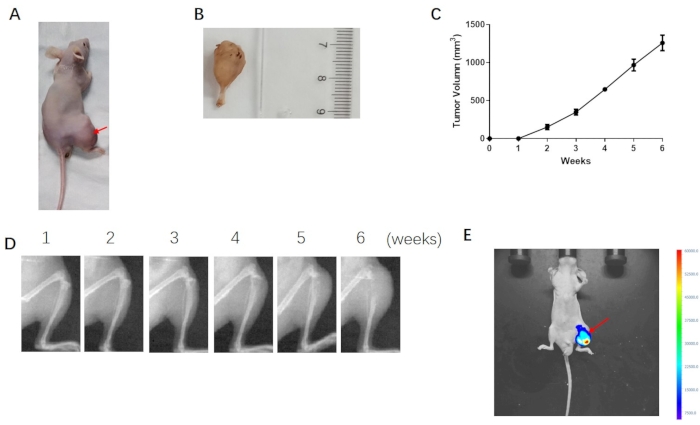
Figure 3: Visualization of the osteosarcoma growth in mice. (A) Successful mouse orthotopic osteosarcoma model. (B) Isolated orthotopic osteosarcoma. (C) Tumor volume was measured with a caliper and calculated using the following formula: tumor volume = 0.5 x longer diameter x short diameter x short diameter. Error bars stand for standard deviation (n = 8). (D) X-ray images were obtained from the same mouse at a different time (from 1-6 weeks). (E) Image obtained on the 28th day after luciferase labeled 143B cells were injected into the mouse tibia. The red arrows indicated the luminescence intensity of the orthotopic (primary) osteosarcoma. Please click here to view a larger version of this figure.
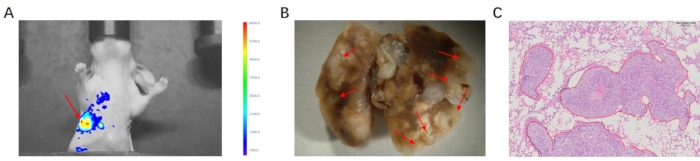
Figure 4: Pulmonary metastasis of osteosarcoma. (A) Image obtained on the 28th day after luciferase labeled 143B cells were injected into the mouse tibia. The red arrows indicated the luminescence intensity of the pulmonary metastasis. (B) The isolated lungs with osteosarcoma metastases. The red arrows indicated the metastatic colonies (x20). (C) H&E staining showed metastatic lesions in lung tissues (scale bar = 200 µm). Please click here to view a larger version of this figure.
Discussion
Orthotopic injection of osteosarcoma cells is an ideal model to study the function and mechanism of specific factors in osteosarcoma carcinogenesis and development to evaluate the therapeutic efficacy. To avoid differences in tumor growth, most active osteosarcoma cells at 80%-90% confluent with the same number are carefully injected into the tibia of each mouse, and the cell trypsinization time is strictly controlled without affecting the cell viability. As cell clumps affect cell counting leading to inaccurate cell numbers being injected into the tibia of each mouse, the cell suspension needs to be appropriately mixed up and down with a pipette to avoid the formation of cell clumps.
Another critical aspect that must be taken into consideration is the resuspended solution for osteosarcoma cells. The injected cells are resuspended in a basement membrane matrix instead of in PBS or culture medium. Moreover, a high concentration of basement membrane matrix is challenging to be pipetted and affects the accurate volume; thus, an appropriate concentration of basement membrane matrix is required26. To drill a hole through the tibia platform for osteosarcoma cell injection, the needling moves forward with the syringe rotation rather than being directly pushed forward until about half of the needle is in the tibia. More particularly, immunodeficient mice are applied to establish an orthotopic osteosarcoma model using human osteosarcoma cells27. Meanwhile, the injection procedure is performed in biological safety cabinet using sterile surgical tools. Since mice may experience uneasiness after anesthesia and surgery, the mice must be closely monitored on the first week postsurgery.
Intratibia injection of osteosarcoma cells labeled with fluorescent protein or luciferase enables the tracking of primary and metastatic lesions using optical imaging28. Osteosarcoma is never allowed beyond the size limit as in the IACUC-approved protocol; meanwhile, ulcerations may occur in enormous size tumor mass, which may lead to failed immunohistochemical analyses. Although the primary bone tumors and bone metastasis have been recently reported to be achieved by implantation of solid tumor graft into bone, and the animals developed reproducible growth, as well as lung metastasis eventually29; however, the authors directly implanted fresh or cryopreserved tumor fragments into the proximal tibia, which showed the disadvantage of open surgery caused potential infection and failure of developing tumor engraftment. Moreover, the volume of implanted tumor fragments without strict control will result in a significant difference in produced tumor volume, which is difficult in following application, such as evaluating the therapeutic efficacy in vivo. Here, a simple and reproducible technique is reported to establish the intratibia primary osteosarcoma with later pulmonary metastasis mouse models via intratibia injection of osteosarcoma cells. This showed the advantages of best mimicking the clinical development characteristics of osteosarcoma in humans; accurate numbers of osteosarcoma cells being directly injected into tibia using micro-volume syringe allowing identical tumor formation rate (100%) and tumor volume. The method ensures avoiding the possibilities of infection or even death using open surgery techniques and allowing lively monitor and quantifying osteosarcoma growth and metastasis using the bioluminescence live imaging system after the injected osteosarcoma cells are labeled with bioluminescence. This prevents the injected osteosarcoma cells from directly reaching the bloodstream and colonizing in the lungs to form pulmonary embolism and/or false-positive pulmonary metastasis by resuspending the injected osteosarcoma cells in appropriate concentration of basement membrane matrix since the basement membrane matrix has the property of coagulation above room temperature. The immediate coagulation support and restrict osteosarcoma cells within the basement membrane matrix after being injected into the mouse tibia.
Another literature has reported the bone metastasis model establishment by intracardiac inoculation or intratibial inoculation of breast cancer cells30; however, cells used in this literature are breast cancer cells, which have different biological and clinical characteristics with osteosarcoma cells; moreover, both the intracardiac and the intratibial inoculation established cancer models in bone are formed by cancer cell colonizing directly or reaching through bloodstream rather than metastasis lesions formed by cancer cell dissemination from the primary cancer lesions.
There are several limitations of the current protocol. Mice used in this protocol are genetic immune system defect nude mice without thymus that prevents them from immunologically rejecting human cells and are widely used in preclinical trials, which are not applicable for immune functional research. Furthermore, we found that not all osteosarcoma cell lines are identically relevant in these models, and the tumorigenesis abilities of 143B, MNNG, MG-63, and U-2 OS cells are higher than the Saos-2 cells.
In conclusion, the present primary and pulmonary metastatic osteosarcoma models generated by orthotopic osteosarcoma cell injection are handy tools to study the tumor microenvironment, efficacy of therapeutics on osteosarcoma growth and/or metastasis. In addition, by intratibia injection of the genetically modified osteosarcoma cells specifically targeting a gene, the models are helpful to explore the key oncogenes and tumor suppressors in osteosarcoma growth and pulmonary metastasis.
Divulgations
The authors have nothing to disclose.
Acknowledgements
This study was supported by grants from (1) National Key R&D Program of China (2018YFC1704300 and 2020YFE0201600), (2) National Nature Science Foundation (81973877 and 82174408).
Materials
| Automatic cell counter | Shanghai Simo Biological Technology Co., Ltd | IC1000 | Counting cells |
| Anesthesia machine | Shenzhen RWD Life Technology Co., Ltd | R500IP | The Equipment of Anesthesia mice |
| BALB/c athymic mice | Shanghai SLAC Laboratory Animal Co, Ltd. | / | animal |
| Basement Membrane Matrix | Shanghai Uning Bioscience Technology Co., Ltd | 356234, BD, Matrigel | re-suspende cells |
| Bioluminescence imaging system | Shanghai Baitai Technology Co., Ltd | Vieworks | tracking the tumor growth and pulmonary metastasis, if the injection cell is labeled by luciferase |
| Centrifuge tube (15 mL) | Shanghai YueNian Biotechnology Co., Ltd | 430790, Corning | Centrifuge the cells |
| isoflurane | Shenzhen RWD Life Technology Co., Ltd | VETEASY | Anesthesia mice |
| MEM media | Shanghai YueNian Biotechnology Co., Ltd | LM-E1141 | Cell culture medium |
| Micro-volume syringe | Shanghai high pigeon industry and trade Co., Ltd | 0-50 μL | Inject precise cells into the tibia |
| Phosphate-buffered saline | Beyotime Biotechnology | ST447 | wash the human osteosarcoma cells |
| 1ml syringes | Shandong Weigao Group Medical Polymer Co., Ltd | 20200411 | drilling |
| 143B cell line | ATCC | CRL-8303 | osteosarcoma cell line |
| Trypsin (0.25%) | Shanghai YueNian Biotechnology Co., Ltd | 25200056, Gibco | trypsin treatment of cells |
| Trypan blue | Beyotime Biotechnology | ST798 | Staining cells to assess activity |
| vector (pLV-luciferase) | Shanghai YueNian Biotechnology Co., Ltd | VL3613 | Plasmid |
| Lipofectamine 2000 | Shanghai YueNian Biotechnology Co., Ltd | 11668027,Thermo fisher | Plasmid transfection reagent |
| X-ray imaging system | Brook (Beijing) Technology Co., Ltd | FX PRO | X-ray images were obtained to detect tumor growth |
References
- Bielack, S. S., et al. Prognostic factors in high-grade osteosarcoma of the extremities or trunk: an analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. Journal of Clinical Oncology. 20 (3), 776-790 (2002).
- Yang, C., et al. Bone microenvironment and osteosarcoma metastasis. International Journal of Molecular Sciences. 21 (19), (2020).
- Mirabello, L., Troisi, R. J., Savage, S. A. Osteosarcoma incidence and survival rates from 1973 to 2004: data from the Surveillance, Epidemiology, and End Results Program. Cancer. 115 (7), 1531-1543 (2009).
- Zhang, B., et al. The efficacy and safety comparison of first-line chemotherapeutic agents (high-dose methotrexate, doxorubicin, cisplatin, and ifosfamide) for osteosarcoma: a network meta-analysis. Journal of Orthopaedic Surgery and Research. 15 (1), 51 (2020).
- Tsukamoto, S., Errani, C., Angelini, A., Mavrogenis, A. F. Current treatment considerations for osteosarcoma metastatic at presentation. Orthopedics. 43 (5), 345-358 (2020).
- Aljubran, A. H., Griffin, A., Pintilie, M., Blackstein, M. Osteosarcoma in adolescents and adults: survival analysis with and without lung metastases. Annals of Oncology. 20 (6), 1136-1141 (2009).
- Ek, E. T., Dass, C. R., Choong, P. F. Commonly used mouse models of osteosarcoma. Critical Reviews in Oncology/Hematology. 60 (1), 1-8 (2006).
- Castillo-Tandazo, W., Mutsaers, A. J., Walkley, C. R. Osteosarcoma in the post genome era: Preclinical models and approaches to identify tractable therapeutic targets. Current Osteoporosis Reports. 17 (5), 343-352 (2019).
- Mason, N. J. Comparative immunology and immunotherapy of canine osteosarcoma. Advances in Experimental Medicine and Biology. 1258, 199-221 (2020).
- Cobb, L. M. Radiation-induced osteosarcoma in the rat as a model for osteosarcoma in man. British Journal of Cancer. 24 (2), 294-299 (1970).
- Walkley, C. R., et al. Conditional mouse osteosarcoma, dependent on p53 loss and potentiated by loss of Rb, mimics the human disease. Genes & Development. 22 (12), 1662-1676 (2008).
- Entz-Werlé, N., et al. Targeted apc;twist double-mutant mice: a new model of spontaneous osteosarcoma that mimics the human disease. Translational Oncology. 3 (6), 344-353 (2010).
- Erstad, D. J., et al. Orthotopic and heterotopic murine models of pancreatic cancer and their different responses to FOLFIRINOX chemotherapy. Disease Models & Mechanisms. 11 (7), (2018).
- Chang, J., et al. MicroRNAs for osteosarcoma in the mouse: a meta-analysis. Oncotarget. 7 (51), 85650-85674 (2016).
- Maloney, C., et al. Intratibial injection causes direct pulmonary seeding of osteosarcoma cells and is not a spontaneous model of metastasis: A mouse osteosarcoma model. Clinical Orthopaedics and Related Research. 476 (7), 1514-1522 (2018).
- Yu, Z., et al. Establishment of reproducible osteosarcoma rat model using orthotopic implantation technique. Oncology Reports. 21 (5), 1175-1180 (2009).
- Fidler, I. J., Naito, S., Pathak, S. Orthotopic implantation is essential for the selection, growth and metastasis of human renal cell cancer in nude mice [corrected]. Cancer Metastasis Reviews. 9 (2), 149-165 (1990).
- Leacock, S. W., et al. A zebrafish transgenic model of Ewing’s sarcoma reveals conserved mediators of EWS-FLI1 tumorigenesis. Disease Models & Mechanisms. 5 (1), 95-106 (2012).
- Sharma, S., Boston, S. E., Riddle, D., Isakow, K. Osteosarcoma of the proximal tibia in a dog 6 years after tibial tuberosity advancement. The Canadian Veterinary Journal. 61 (9), 946-950 (2020).
- Mohseny, A. B., Hogendoorn, P. C. Zebrafish as a model for human osteosarcoma. Advances in Experimental Medicine and Biology. 804, 221-236 (2014).
- Hu, S., et al. Cantharidin inhibits osteosarcoma proliferation and metastasis by directly targeting miR-214-3p/DKK3 axis to inactivate β-catenin nuclear translocation and LEF1 translation. International Journal of Biological Sciences. 17 (10), 2504-2522 (2021).
- Chang, J., et al. Polyphyllin I suppresses human osteosarcoma growth by inactivation of Wnt/β-catenin pathway in vitro and in vivo. Scientific Reports. 7 (1), 7605 (2017).
- Lamar, J. M., et al. SRC tyrosine kinase activates the YAP/TAZ axis and thereby drives tumor growth and metastasis. The Journal of Biological Chemistry. 294 (7), 2302-2317 (2019).
- Benton, G., Arnaoutova, I., George, J., Kleinman, H. K., Koblinski, J. Matrigel: from discovery and ECM mimicry to assays and models for cancer research. Advanced Drug Delivery Reviews. , 3-18 (2014).
- Chang, J., et al. Matrine inhibits prostate cancer via activation of the unfolded protein response/endoplasmic reticulum stress signaling and reversal of epithelial to mesenchymal transition. Molecular Medicine Reports. 18 (1), 945-957 (2018).
- Fridman, R., et al. Enhanced tumor growth of both primary and established human and murine tumor cells in athymic mice after coinjection with Matrigel. Journal of the National Cancer Institute. 83 (11), 769-774 (1991).
- Kocatürk, B., Versteeg, H. H. Orthotopic injection of breast cancer cells into the mammary fat pad of mice to study tumor growth. Journal of Visualized Experiments. (96), e51967 (2015).
- Paschall, A. V., Liu, K. An orthotopic mouse model of spontaneous breast cancer metastasis. Journal of Visualized Experiments. (114), e54040 (2016).
- Hildreth, B. E., Palmer, C., Allen, M. J. Modeling primary bone tumors and bone metastasis with solid tumor graft implantation into bone. Journal of Visualized Experiments. (163), e61313 (2020).
- Campbell, J. P., Merkel, A. R., Masood-Campbell, S. K., Elefteriou, F., Sterling, J. A. Models of bone metastasis. Journal of Visualized Experiments. (67), e4260 (2012).
