Laser Doppler flowmetry (LDF) was used to monitor rCBF during induction of cerebral ischemia6,7. Many laboratories including our laboratory have been using rCBF to identify animals with successful MCA occlusion, but the thresholds of baseline varied between laboratories which are related to the site of measurement. The probe of the LDF is positioned at 2 mm posterior and 5 mm lateral to the bregma as described previously6. rCBF was monitored at 0, 5, 15, 30, 60, 90, and 120 min after injection of the clot. On the basis of this data, only animals that exhibit a reduction in rCBF >70% of baseline are considered successful embolic occlusion of the MCA (Figure 5). At 2 hr after injection of clot, a standard rat dose of tPA (10 mg/kg)7,8 was administered intravenously with a 10% bolus and 90% continuous infusion over 30 min using a syringe infusion pump7,8. We observed that rCBF levels gradually increased to >70% of the baseline within 30 min of tPA therapy (Figure 5).
At 24 hr after embolization, the animals were euthanized and transcardially perfused with 200 ml of PBS to remove intravascular blood. Previous studies2,3,7,8 and our data (Figure 6) have shown substantially larger tissue infarctions produced at 24 hr after embolization. The brains were collected and taken pictures. In saline-treated group, the blood clot was readily visualized at the origin of the MCA and ACA, but the clot was almost completely dissolved in tPA-treated group (Figure 6A). After that, the brain was sliced into seven 2 mm coronal sections with a rat brain matrix on ice. Incubate the brain slices in 2% 2,3,5-triphenyltetrazolium chloride (TTC) at 37 °C for 30 min9,10. After TTC staining, the coronal sections were placed on a plate and photographed (Figure 6B). The area of infarction in each slice was determined by the computerized image analysis system (National Institutes of Health Image), and the average infarct volume was calculated by multiplying the distance between sections. This embolic stroke model produced tissue infarction within the MCA territory as seen in the neocortex and striatum regions (Figure 6B). Early reperfusion was established by intravenous administration of tPA at 2 hr after embolization, the infarct volumes were significantly reduced in the tPA-treated group (229.1 ± 45.7 mm3, n = 12) compared with the saline-treated group (394.2 ± 68.2 mm3, n = 9) (P < 0.01). The 24 hr mortality rate is 16% (4/25).
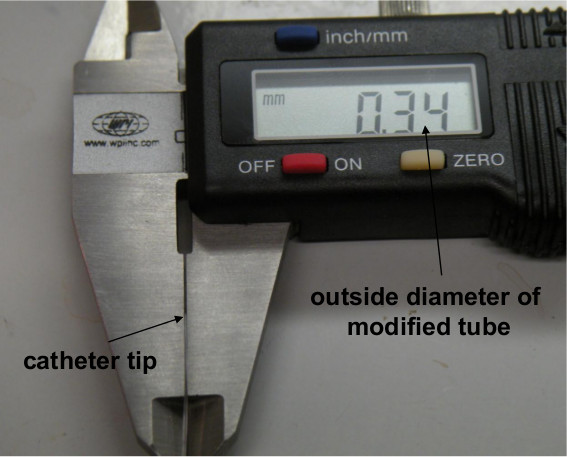
Figure 1. Measurement of the outside diameter of the modified PE-50 tube using a digital caliper.
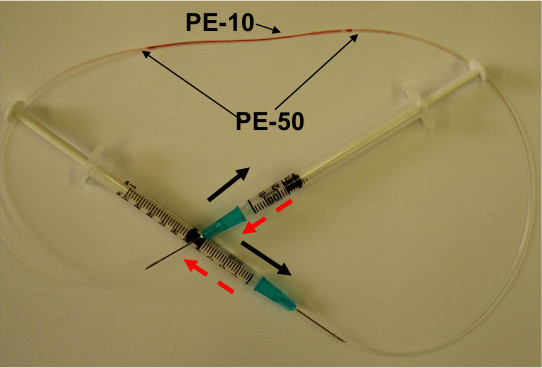
Figure 2. Washing blood clot in a PE-10 tube. The blood clot was washed by alternative pushing the two syringes connected to the end of PE-50 tube.
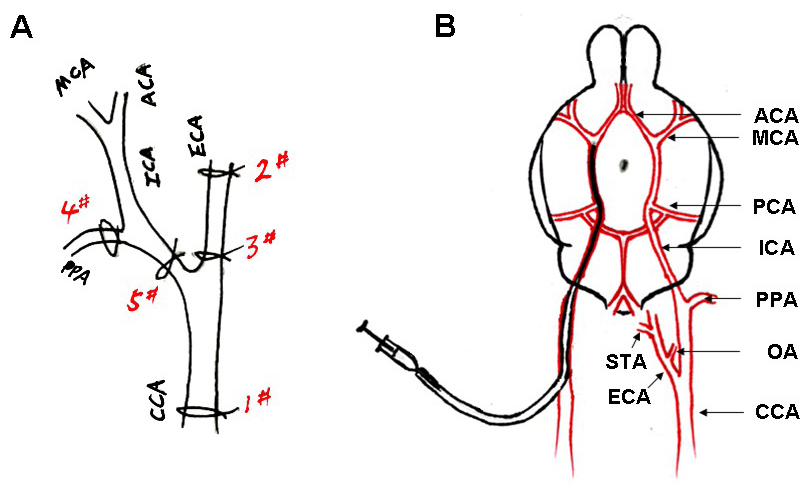
Figure 3. (A) Simplified scheme of rat right hemisphere isolated arteries showing successive sutures to prepare the introduction of modified PE-50 tube. (B) Scheme of the arterial architecture in the rat brain, and the catheter advanced from the ECA to the ICA of the rat. A single blood clot (black) was contained in the tube.
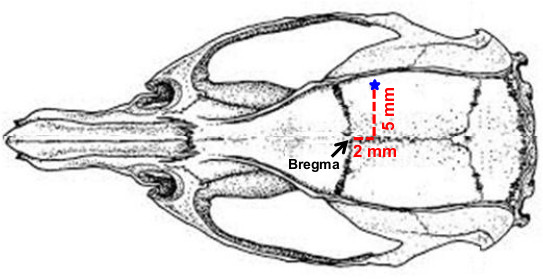
Figure 4. The burr hole (1.5 mm diameter) located at 2 mm posterior and 5 mm lateral to the bregma.
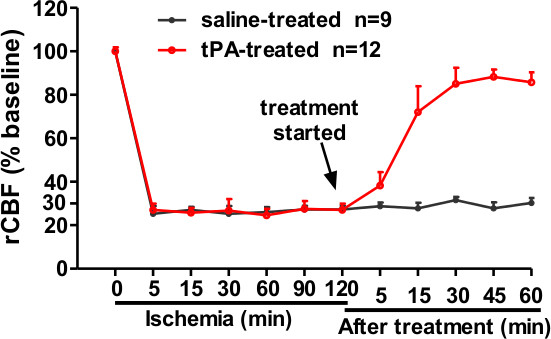
Figure 5. Regional cerebral blood flow (rCBF) was measured using a laser Doppler flowmeter (LDF). The clot injection led to >70% rCBF reduction of the baseline value. tPA (10 mg/kg) treated at 2 hr after the clot injection restored rCBF close to baseline after 30 min of tPA treatment. Data was expressed as mean ± SD.
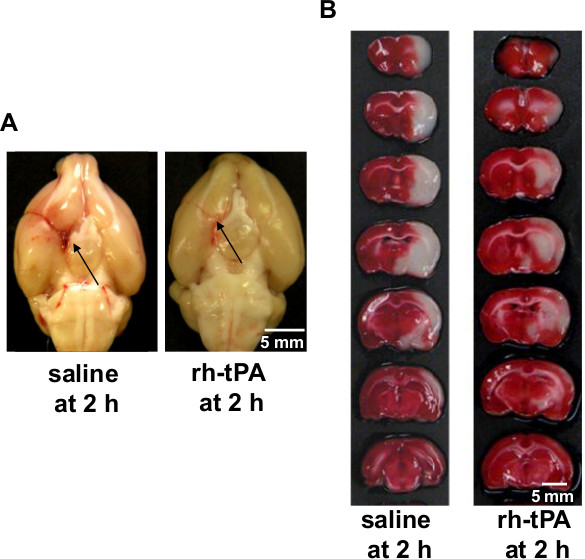
Figure 6. (A) Representative pictures showing the blood clots (black arrows) in the origin of the middle cerebral artery (MCA) and anterior cerebral artery (ACA) at 24 hr after stroke. Left, saline-treated rat; Right, tPA-treated rat, bar = 5 mm. (B) Representative images showing TTC-stained brain slices at 24 hr after stroke. Left, saline-treated rat; Right, tPA-treated rat, bar = 5 mm.
