Since 2009, our pituitary program has evolved to a point where a fully endoscopic endonasal approach has been used to treat pituitary tumors with excellent postoperative results. From 2009 to 2016, the two senior surgeons (RTD and MM) operated on 473 patients with pituitary adenomas through a full endoscopic technique. The histology is detailed in Table 1: most of these cases were non-functioning pituitary adenomas (57%) (Figure 1), followed by growth hormone (GH)-secreting adenoma (Figure 4) and adrenocorticotrophic hormone (ACTH)-secreting adenomas (20% and 17%, respectively).
The resection rate was related to the histology of the pituitary tumors, the size, and the invasiveness of the cavernous sinus and sphenoid sinus, thus confirming the data of literature on this subject18. We achieved a total resection in 80% of patients with non-functioning pituitary tumors (Figure 1). When stratifying adenomas according to their invasiveness, a total resection rate was obtained in 90% of cases with no cavernous sinus invasion, while it lowered to 67% when the cavernous sinus was invaded.
For secreting pituitary adenomas, the resection rate was variable and in some cases discordance was observed between the postoperative imaging and the endocrinological remission. Data reporting the postoperative endocrinological results according to tumor type are reported in Table 2. In this data, the relationship between the size of the tumor and its parasellar extension is evident. The biological remission varied from 90% for GH-secreting microadenomas to 30% with GH-secreting macroadenomas with cavernous sinus invasion (Figure 4). For ACTH adenomas, the remission was achieved in 55% of cases of macroadenoma and in 90% of microadenomas.
When considering the ophthalmological outcome, we observed normalization or improvement of visual acuity and visual field size in 95% of patients with preoperative deficits. Five per cent of patients showed a stabilization of their visual status in the postoperative period. With regards to surgical morbidity, the overall mortality rate was less than 0.2% (one acromegalic patient died 1 month after surgery because of an ICA pseudo aneurysm). A CSF leak was observed in 8% of patients in the early part of the surgical series (2008-2011). The rate of this complication subsequently decreased to less than 1% with the adoption of a multilayer sellar floor reconstruction (2011-2016).
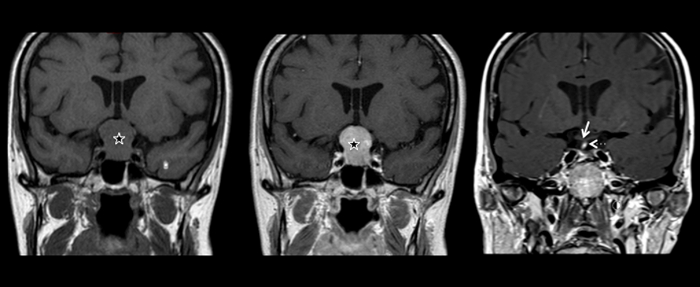
Figure 1: Coronal views of the cerebral MRI of one patient with non-functioning pituitary macroadenoma with a large suprasellar extension.
In the left panel, a T1-weighted MRI illustrates the sellar lesion (star) enlarging the sellar fossa and with a mass effect on the optic chiasm. The image of the central panel illustrates the same lesion after gadolinium administration: a diffuse contrast enhancement is present in the tumor and the normal hypophysis is not visible. The postoperative control is reported in the right panel: a complete resection of the macroadenoma was possible through a full-endoscopic endonasal procedure. The normal pituitary is now visible in the sella, as well as the pituitary stalk, which appears slightly deviated to the right (hyperintense in the T1-weighted MRI, dotted arrow). The optic chiasm is returned to its normal position (white arrow). Please click here to view a larger version of this figure.
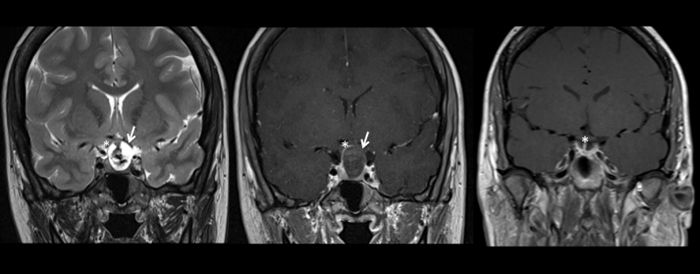
Figure 2: Coronal views of a cerebral MRI showing a pituitary apoplexy (left and central panel) with its postoperative control (right panel).
A T2-weighted MRI is reported in the left panel, confirming an enlarged sella containing a large lesion with a heterogenous signal confirming a hemorrhagic transformation (white arrow).
In the central panel, a T1-weighted MRI with gadolinium administration shows a lesion with an important suprasellar extension, with a peripheral contrast enhancement, and a central core which appears hypointense. The optic chiasm is displaced (white asterisk indicating the right optic nerve; the left optic nerve is hardly visible because of the compression) and the patient presented thunderclap headaches and sudden visual loss in the left eye. He was urgently operated through an endoscopic endonasal approach and the results are shown in the right panel: the hemorrhagic macroadenoma was completely resected (right panel). The patient had a persistent anterior pituitary insufficiency but he completely recovered from the visual deficit. The optic chiasm is visible in its normal position (white asterisk in the right panel) Please click here to view a larger version of this figure.
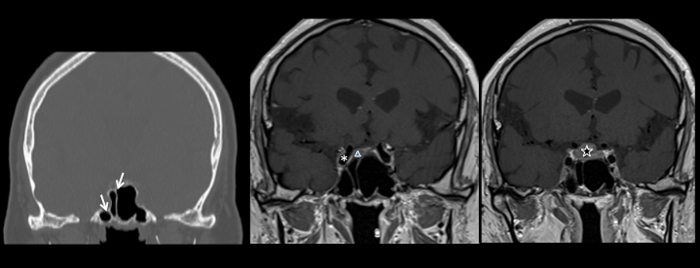
Figure 3: Multiple examples illustrating the pneumatization and the septa orientation of the sphenoid sinus. The sphenoid septum is classically described as median but many variants may occur and the examples illustrated here shows asymmetric septa to underline the utility of a careful analysis of the preoperative CT and MRI.
In the left panel, a coronal view of the CT scan shows the presence of two septa in the sphenoidal sinus, lateralized toward the right side and even dividing the right lateral recess from the rest of the sinus (white arrows). In the middle and right panels, T1-weighted cerebral MRIs with contrast administration are reported. Septa may guide the surgeon toward the pituitary, the tumors, or the internal carotid artery (the right internal carotid artery is marked with an asterisk in the central panel; a micro and a macroadenoma are marked with a triangle and a star in the central and right panel, respectively). A good orientation is thus fundamental to correctly performing the procedure, achieving a maximal resection of the tumor, and avoiding complications, such as vascular injuries. An intraoperative neuronavigation may help in the management of cases with a complex anatomy. Please click here to view a larger version of this figure.
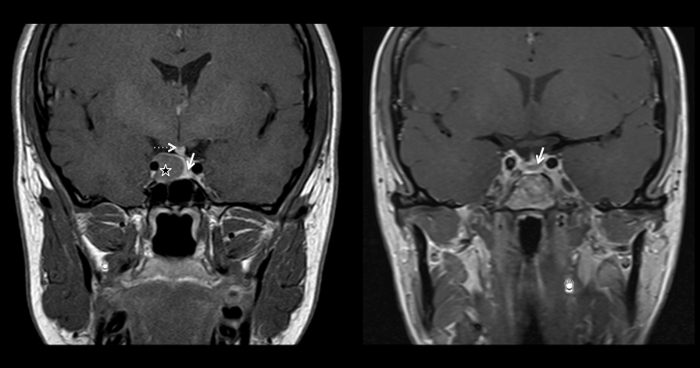
Figure 4: Preoperative (left panel) and postoperative (right panel) T1-weighted cerebral MRI with gadolinium administration in the coronal plane. In the left panel, a well circonscribed lesion is visible in the right side of the sellar fossa (star), hypointense after contrast administration when compared to the normal pituitary, which is displaced to the left (white arrow). The pituitary stalk is also deviated to the left (dotted arrow). In the right panel, the postoperative control is reported, showing a complete resection of the macroadenoma (normal pituitary visible in the sellar fossa, indicated by the white arrow). The patient presented with clinical signs and symptoms of acromegaly, and the lesion was a GH-secreting pituitary adenoma. After the excision, IGF-1 descended to the normal range and a close follow-up was organized. Please click here to view a larger version of this figure.
| Type of Adenoma | Number of Patients |
| Total 473 (%) | |
| GH adenoma (Acromegaly) | 95 (20) |
| ACTH adenoma (Cushing's disease) | 80 (17) |
| PRL adenoma | 24 (5) |
| TSH adenoma | 3 (0.6) |
| Non-functioning adenomas | 271 (57.4) |
Table 1: Endoscopic endonasal surgery for Pituitary adenomas: Personal Case Summary (2009-2016). This table shows the distribution of the 473 pituitary adenomas operated between 2009 and 2016 according to the pathology. In 57% of cases they were non-functioning pituitary adenomas, in 20% GH-secreting adenomas while in 17% ACTH-secreting adenomas. Only 5% were PRL-secreting adenomas, because of the high rate of good outcomes with a medical treatment. TSH-secreting adenomas were rare (3 cases).
| Type of Adenoma | Remission (follow up at 7 years) |
| GH Microadenomas without CS invasion | 90% |
| GH Macroadenomas without CS invasion | 65% |
| GH Macroadenomas with CS invasion | 30% |
| PRL | 55% |
| ACTH Microadenoma | 90% |
| ACTH Macroadenoma | 55% |
| TSH | 100% |
Table 2: Endocrinological results of endoscopic endonasal surgery for Functional pituitary adenomas. The endocrinological outcome varied according to the histology of the pituitary adenoma, its size and radiological invasiveness, defined as cavernous sinus invasion at the cerebral MRI. A complete remission was obtained in the 3 cases of thyrotropinomas and in 90% of ACTH-secreting and GH-secreting microadenomas. A lower remission rate was obtained with GH-secreting and ACTH-secreting macradenomas and with GH-adenomas invading the cavernous sinus.
