Hemodynamic and Physiological Parameters:
The MAP decreased immediately after the hemorrhage (Figures 3A – 3D). During the balloon inflation phase, animals in the complete occlusion group experienced a higher proximal MAP compared to the animals in the partial occlusion group (Figures 3A and 3B). The average distal MAP during the balloon inflation was higher in the partial occlusion group compared to the complete occlusion group (average distal MAP, balloon inflation phase; partial: 31 ± 2.9 mmHg, complete: 16.5 ± 1.14 mmHg; p > 0.05), reflecting the partial distal aortic flow (Figures 3C and 3D). Following resuscitation, the proximal and distal MAPs increased in both groups and returned to the baseline following the balloon deflation for the remainder of the critical care phase (Figures 3A – 3D).
All animals experienced reflex tachycardia immediately following the hemorrhage, which underwent an incremental increase during the balloon inflation phase in both groups (Figure 4A). Following the balloon deflation, the HRs were significantly higher for the remainder of the critical care phase in the complete occlusion group compared to the partial occlusion group, although this difference in HR was not statistically significant.
Following the hemorrhage, the CVP decreased in both groups (Figure 4B). It underwent a rising trend following the balloon inflation. Following the balloon deflation, the complete occlusion group demonstrated a greater decrease in CVP compared to the partial occlusion group, although not statistically different. Following the additional resuscitation in the critical care phase, the CVP recovered toward the baseline in both groups. Similarly, the CO decreased following the hemorrhage, increased during the balloon inflation, and returned to the baseline following the balloon deflation and resuscitation for both groups (Figure 4C).
The carotid flow decreased in both groups immediately following the hemorrhage (Figure 4D). Following the balloon inflation, the complete occlusion group demonstrated higher carotid flow rates compared to the partial occlusion group. Following the resuscitation and balloon deflation, the carotid flow rate recovered toward the baseline in both groups. However, this carotid flow was lower in the complete occlusion group as compared to the partial occlusion group.
Laboratory Parameters:
No appreciable differences in the baseline pH and lactate level were noted between the groups. Following the balloon inflation, the animals in both groups experienced a decrease in pH (Figure 5A). The pH nadir in the complete occlusion group was notably lower than that in the partial occlusion group (complete: 7.14 ± 0.01, partial: 7.32 ± 0.02, p = 0.1). The lactate level was significantly higher throughout balloon inflation and the remainder of the critical care phase in the complete occlusion group (complete: 17.5 ± 0.71 mmol, partial: 6.1 ± 0.28 mmol, p = 0.03) (Figure 5B). This difference in lactate levels decreased slowly until the levels were similar at the end of the critical care phase.
Resuscitation Requirements:
The total fluid requirement for animals in the complete occlusion group was significantly higher than for the animals in the partial occlusion group (total additional fluid resuscitation for the animals in the complete occlusion group: 47.5 ± 3.4 cm3/kg, total additional fluid resuscitation for the animals in the partial occlusion group: 3.7 ± 0.4 cm3/kg, p = 0.003) (Figure 6A). Similarly, the norepinephrine requirement in the complete occlusion group was significantly higher than in the partial occlusion group (complete: 289.7 ± 25.4 µg/kg, partial: 32 ± 13.8 µg/kg, p = 0.006) (Figure 6B).
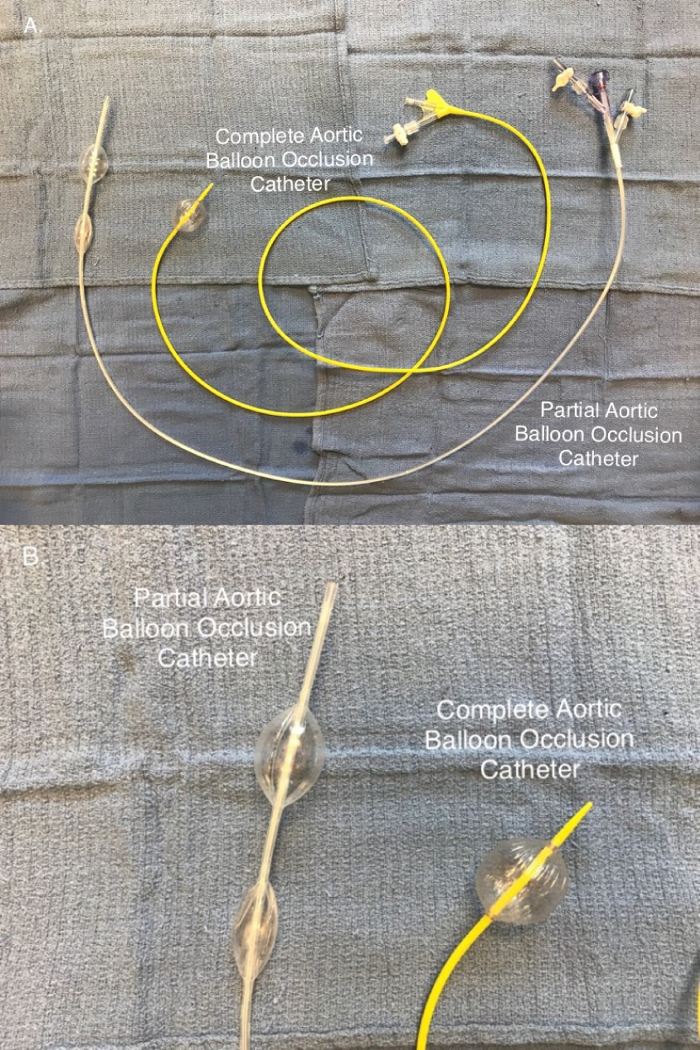
Figure 1: Aortic balloon occlusion catheters. (A) Partial aortic occlusion is achieved using a selective aortic balloon occlusion in trauma (SABOT) catheter, while complete aortic occlusion is achieved using the complete aortic balloon occlusion catheter. (B) The partial aortic balloon occlusion catheter is a two-balloon system that allows an intra-luminal blood flow providing a distal aortic flow. Complete aortic occlusion is provided using a single-balloon system. Please click here to view a larger version of this figure.
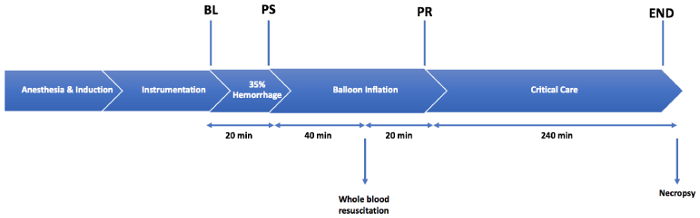
Figure 2: Injury protocol. An injury consisting of a 35% total blood volume hemorrhage is followed by a 1 h period of aortic balloon occlusion. A resuscitation is performed with 20% whole blood over 20 min, after 40 min of balloon occlusion. The animals are monitored in the critical care phase for 4 h following the balloon deflation. BL = the baseline; PS = post-shock; PR = post-resuscitation period. Please click here to view a larger version of this figure.
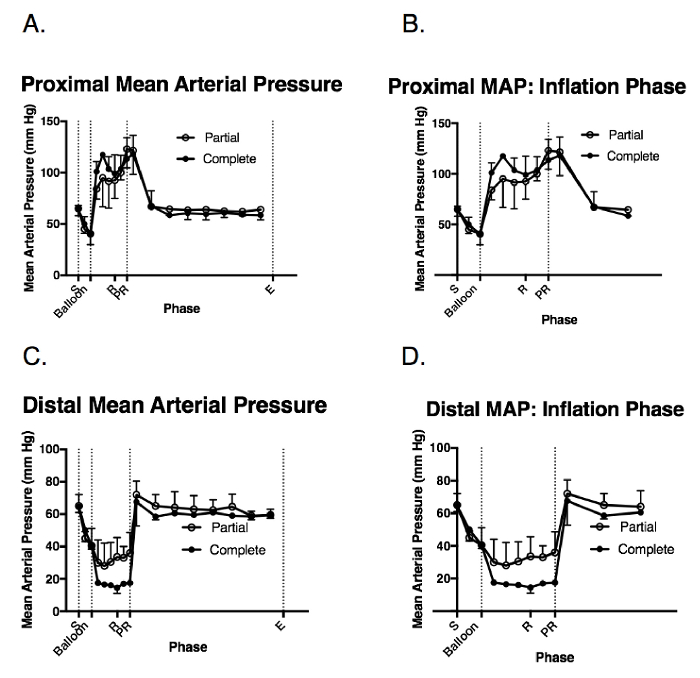
Figure 3: Hemodynamic response to the injury and balloon inflation. These panels show the intraoperative measurements of (A) the proximal pean arterial pressure (MAP), (B) the proximal MAP during the balloon inflation, (C) the distal MAP, and (D) the distal MAP during the balloon inflation. The data are presented as the group mean ± the standard error (SE). S = the shock period (20 min); Balloon = the balloon inflation (60 min); R = the resuscitation (20 min); PR = the post-resuscitation period/balloon deflation; E = the end of the injury phase (5 h following the shock period completion); Complete = the complete aortic balloon occlusion catheter; Partial = the partial aortic balloon occlusion catheter. Please click here to view a larger version of this figure.
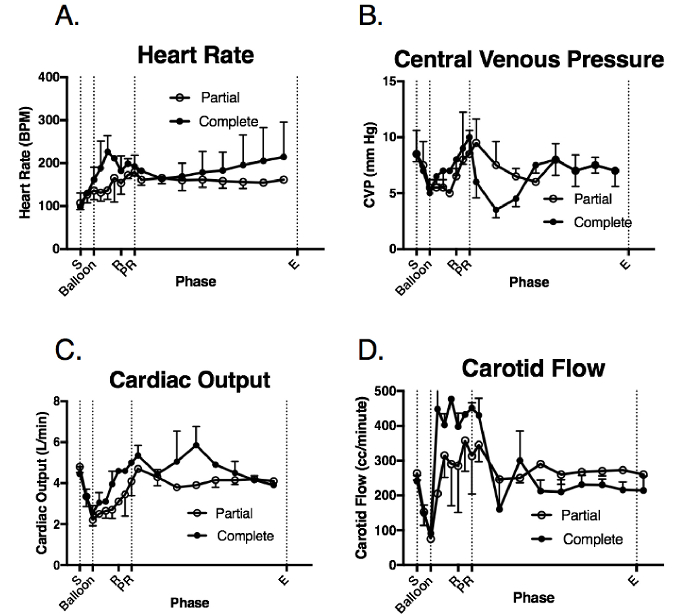
Figure 4: Systemic and physiologic response to the injury and balloon deployment. These panels show the intraoperative measurements of (A) the heart rate (HR), (B) the central venous pressure (CVP), (C) the cardiac output (CO), and (D) the carotid flow (CF). The data are presented as group mean ± SE. S = the shock period (20 min); Balloon = the balloon inflation (60 min); R = the resuscitation (20 min); PR = the post-resuscitation period/balloon deflation; E = the end of the injury phase (5 h following the shock period completion); Complete = the complete aortic balloon occlusion catheter; Partial = the partial aortic balloon occlusion catheter. Please click here to view a larger version of this figure.
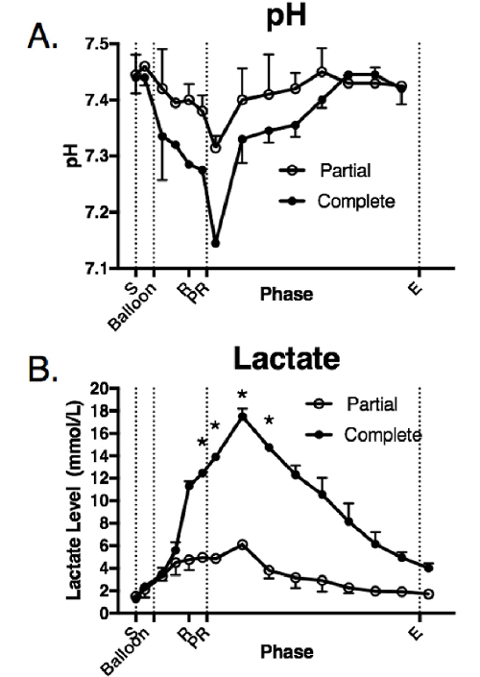
Figure 5: Laboratory parameters in response to the injury and balloon inflation. These panels show the intraoperative measurements of (A) pH and (B) lactate. The data are presented as group mean ± SE. The asterisks indicate the time points that were significantly different (p < 0.05). S = the shock period (20 min); Balloon = the balloon inflation (60 min); R = the resuscitation (20 min); PR = the post-resuscitation period/balloon deflation; E = the end of the injury phase (5 h following the shock period completion). Complete = the complete aortic balloon occlusion catheter; Partial = the partial aortic balloon occlusion catheter. Please click here to view a larger version of this figure.
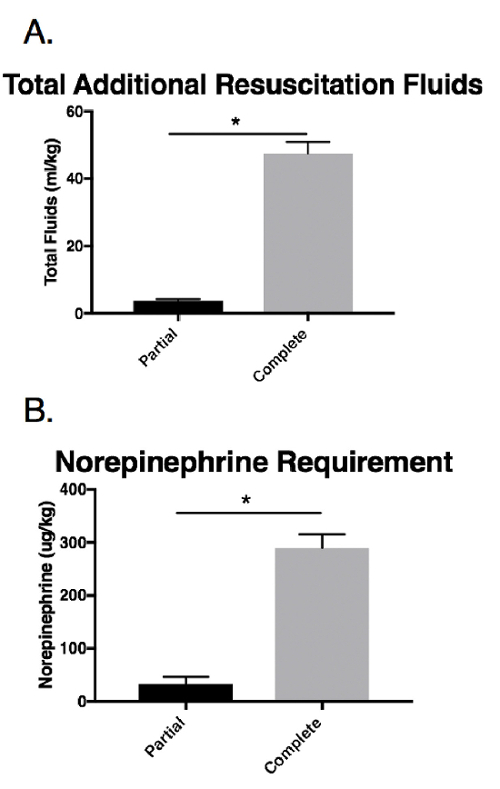
Figure 6: Resuscitation requirements in response to the injury and balloon inflation. These panels show the intraoperative measurements of (A) total additional resuscitation fluids and (B) the norepinephrine use. The data are presented as group mean ± SE. The asterisks indicate significant differences (p < 0.05). Complete = the complete aortic balloon occlusion catheter; Partial = the partial aortic balloon occlusion catheter. Please click here to view a larger version of this figure.
