Individual components of the ultrasound system used in this manuscript are shown in Figure 1. Figure 2 shows representative ultrasound images acquired in B-mode at gd5, 8, 10, and 12 (B) and corresponding implantation area measurement results (A), demonstrating a significant reduced implantation area of anti-CD122-treated Cpa3Cre/+ mice from gd10 onwards.
Figure 3 shows single parts of an implantation (decidua basalis, placenta, embryo) acquired in B-mode (Figure 3A) and conduced placental measurement (area, thickness, diameter) (Figure 3B). Placental measurements resulted in a significantly reduced placental area (Figure 3A), thickness (Figure 3B), and diameter (Figure 3C) in anti-CD122-treated Cpa3Cre/+ mice compared to WTs at gd10 and gd12. In contrast, placental area and diameter were comparable between the groups at gd14, and thickness was significantly increased in anti-CD122-treated Cpa3Cre/+ mice in comparison to WTs at gd14.
Figure 4 shows fetal and placental weight at gd14. Results revealed a significantly decreasedfetal weight (Figure 4A), comparable placental weight (Figure 4B), and significantly decreased feto-placental index (FPI) (Figure 4C) in anti-CD122-treated Cpa3Cre/+ mice compared to WTs. Figure 5 shows a representative PW doppler image of the UA of a WT mouse (Figure 5A) and measurements of peak systolic velocity (PSV) (Figure 5B), end diastolic velocity (EDV) (Figure 5C), and the calculated resistance index (Figure 5D), whereby all values were comparable between the groups. Figure 6 shows a representative color doppler image of a WT fetal UmA at gd14 (Figure 6A) and representative PW doppler images with normal, absent, or reversed end diastolic flow (Figure 6B) and measurements of PVS (Figure 6C), EDV (Figure 6D), systolic/diastolic ratio (Figure 6E), and resistance index (Figure 6F). The resistance index of anti-CD122-treated Cpa3Cre/+ mice was significantly increased compared to WT mice.
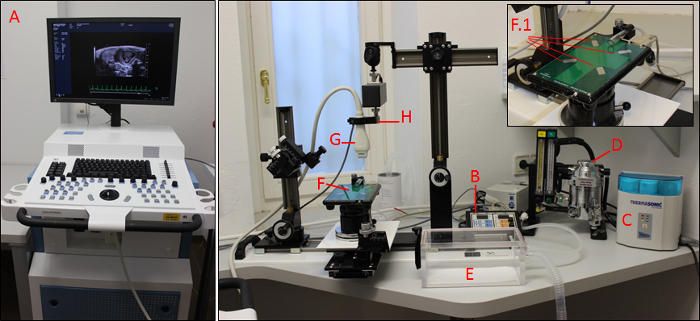
Figure 1: The imaging system. Main control unit (A) with heating platform control pad (B), gel warmer (C), isoflurane control unit (D), knockdown box (E), heated platform with four copper areas (F; F.1), transducer (G), and transducer holding device (H). Please click here to view a larger version of this figure.
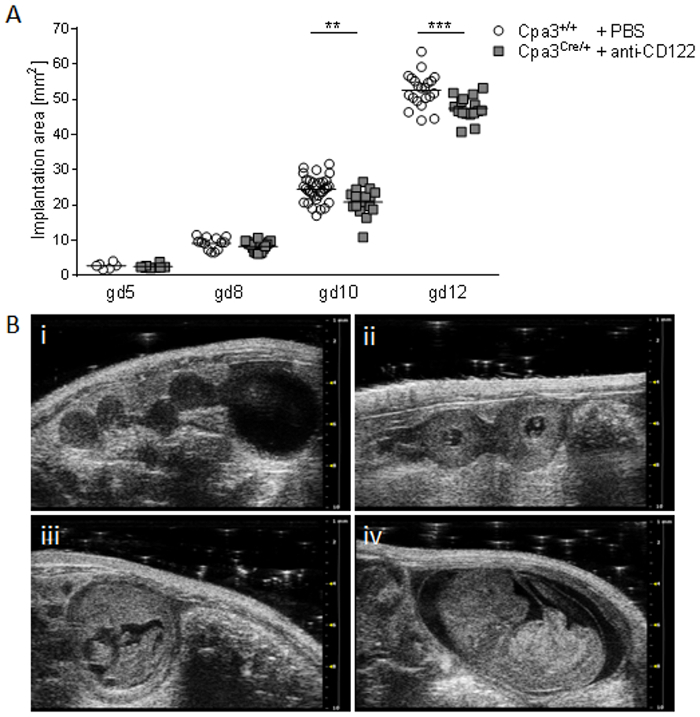
Figure 2: Comparison of implantation areas at gd5, 8, 10, and 12. (A) Implantation areas from WT Cpa3+/+ + PBS mice (mice n = 2-5, implantations n = 6-31 per day) and MC/NK-deficient Cpa3Cre/+ + anti-CD122 mice (mice n = 3, implantations n = 8-16 per day) at gd5, 8, 10, and 12. Results are presented as individual values for each single implantation and mean. Statistical differences were obtained using an unpaired t-test (**p < 0.01, ***p < 0.001). (B) Representative ultrasound images from Cpa3+/+ + PBS mice at gd5 (i), gd8 (ii), gd10 (iii), and gd12 (iv). gd, gestation day; WT, wild type; MC, mast cell; NK, natural killer cell. This figure is republished from a previous publication23. Please click here to view a larger version of this figure.
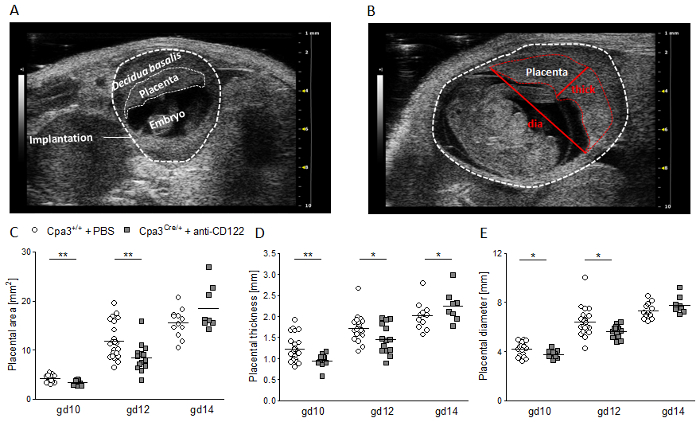
Figure 3: Placental measurements at gd10, 12, and 14. (A) Representative ultrasound image of a WT implantation at gd10 showing the decidua basalis, placenta, and embryo. (B) Representative ultrasound image of a WT implantation at gd12 showing placental thickness (thick) and placental diameter (dia). Placental area (C), placental thickness (D), and placental diameter (e) from WT Cpa3+/+ + PBS mice (mice n = 3-5, placentas n = 12-22 per day) and MC/ NK-deficient Cpa3Cre/+ + anti-CD122 mice (mice n = 3-4, placentas n = 8-14 per day) at gd10, 12, and 14. Results are presented as individual values for each single placenta and mean. Statistical differences were obtained using an unpaired t-test (*p < 0.05, **p < 0.01). gd, gestation day; WT, wild type; thick, thickness; dia, diameter; MC, mast cell; NK, natural killer cell. This figure is republished from a previous publication23. Please click here to view a larger version of this figure.
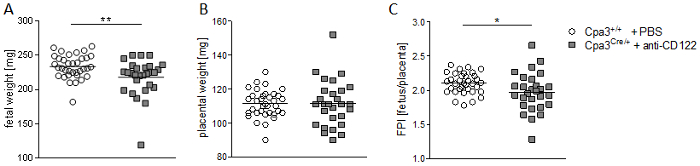
Figure 4: Fetal and placental weight measurements and feto-placental index (FPI) at gd14. Fetal weights (A), placental weights (B), and FPIs (C) from progeny of WT Cpa3+/+ + PBS mice (mice n = 4, fetus/placentas n = 35) and MC/NK-deficient Cpa3Cre/+ + anti-CD122 mice (mice n = 3, fetus/placentas n = 28) at gd14. Results are presented as individual values and mean. Statistical differences were obtained using unpaired t-test (*p < 0.05, **p < 0.01). gd, gestation day; WT, wild type; MC, mast cell; NK, natural killer cell. This figure is republished from a previous publication23. Please click here to view a larger version of this figure.
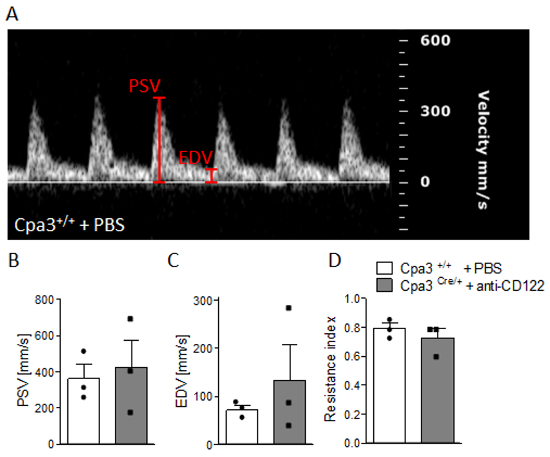
Figure 5: Analysis of uterine artery velocities at gd10. (A) Representative pulse-wave doppler images from WT Cpa3+/+ + PBS mice showing PSV and EDV. PSV (B), EDV (C), and resistance index (D) of uterine arteries from Cpa3+/+ + PBS (n = 3) and Cpa3Cre/+ + anti-CD122 (n = 3) mice at gd10 of pregnancy. Data are presented as mean with SEM. Statistical analysis was performed using the Mann-Whitney U test. gd, gestation day; WT, wild type; MC, mast cell; NK, natural killer cell; PSV, peak systolic velocity; EDV, end diastolic velocity. This figure is republished from a previous publication23. Please click here to view a larger version of this figure.
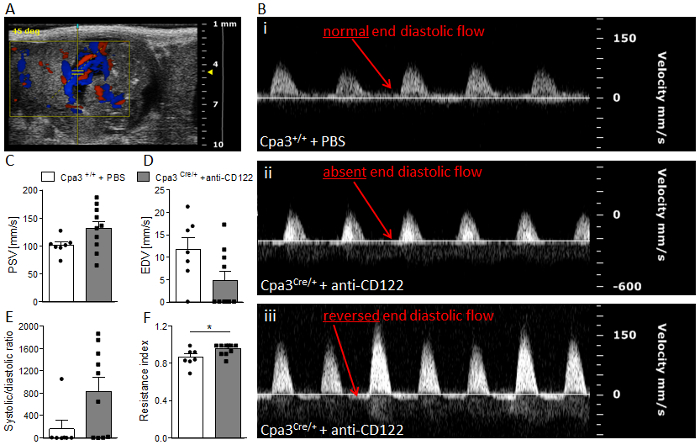
Figure 6: Analysis of umbilical artery velocities at gd14. (A) Representative Color Doppler image of a fetal UmA at gd 14. (B) Representative pulse-wave doppler images from Cpa3+/+ + PBS (i) and Cpa3Cre/+ + anti-CD122 (ii, iii) mice, showing normal end diastolic flow (i), absent end diastolic flow (ii), or reversed end diastolic flow (iii). PSV (C), EDV (D), systolic/diastolic ratio (E), and resistance index (F) of UmAs of fetuses from Cpa3+/+ + PBS (mice n = 3, UmA measurements n = 7) and Cpa3Cre/+ + anti-CD122 (mice n = 3, UmA measurements n = 10) mice at gd14. Data are presented as mean with SEM. Statistical analysis was performed using an unpaired t-test (*p < 0.05). UmA, umbilical artery; gd, gestation day; PSV, peak systolic velocity; EDV, end diastolic velocity. This figure is republished from a previous publication23. Please click here to view a larger version of this figure.
