Once all the elements are in place, the catheter has connectors on almost all the junctions between two infusion lines (Figure 1). Thus, it has proximal connectors on each line and two connectors on the sockets of the 3-way extensions (Figure 2). Each infusion line has connectors at all its female sockets (Figure 3). Once the assembly is in place, any injection or infusion (continuous or discontinuous) must be made, after disinfection, through one of the connectors of the infusion lines or extensions (Figure 4).
Maintaining the connectors in place keeps the infusion system closed as well as sterile mounted and minimizes the risk of bacterial contamination. One of our previous works, the first study that prospectively analyzed these devices over several years, showed a significant decrease in CRI incidence during the six-year period framing the introduction of the connectors (Figure 5)10. In this work, the incidence of CRI before using connectors was 6.2 CRI/1000 catheter-day vs. 2.7 CRI/1000 catheter-days after using connectors10. Moreover, we did not find any increase of CRI after the beginning of connector use (Figure 5) and there was no significant difference concerning the kind of bacteria species involved in CRI10. We have not identified any specific complications associated with the use of these connectors during these years of use.
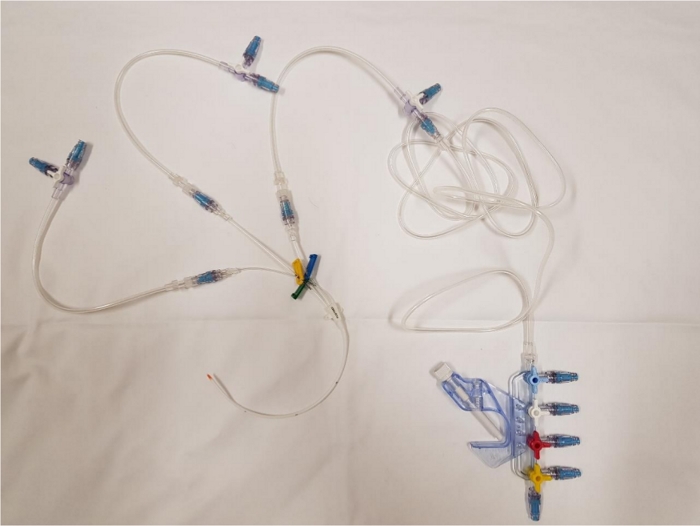
Figure 1: Global view of the catheter once the connectors have been placed. Please click here to view a larger version of this figure.
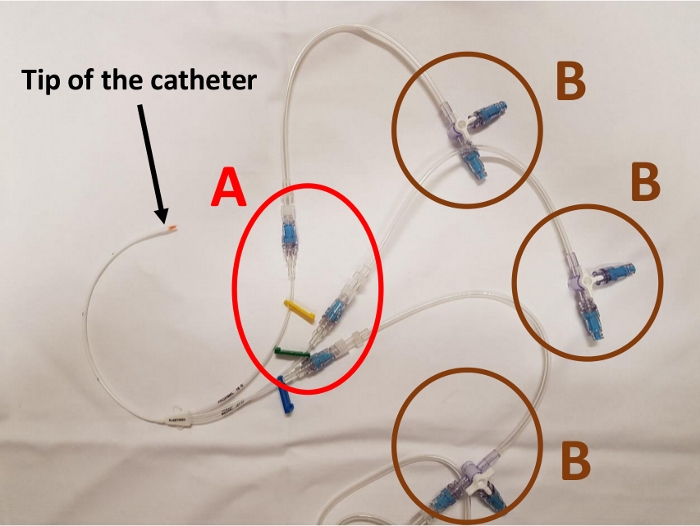
Figure 2: Proximal part of the catheter with proximal connectors (A) and connectors on the 3-way extension stopcock (B). Please click here to view a larger version of this figure.

Figure 3: 4-port manifold with connectors. Please click here to view a larger version of this figure.
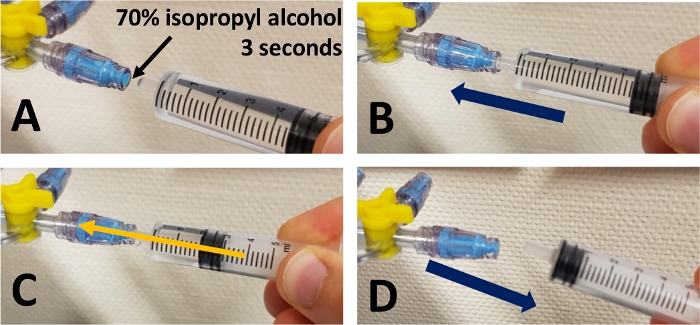
Figure 4: Steps of injection through a connector. (A) Disinfect the surface of the connector for 3 seconds with 70% isopropyl alcohol. Wait until the connector is dry. (B) Insert the tip of the syringe or infuser into the connector. (C) Inject or infuse the medication. (D) Remove the syringe or infuser. Please click here to view a larger version of this figure.
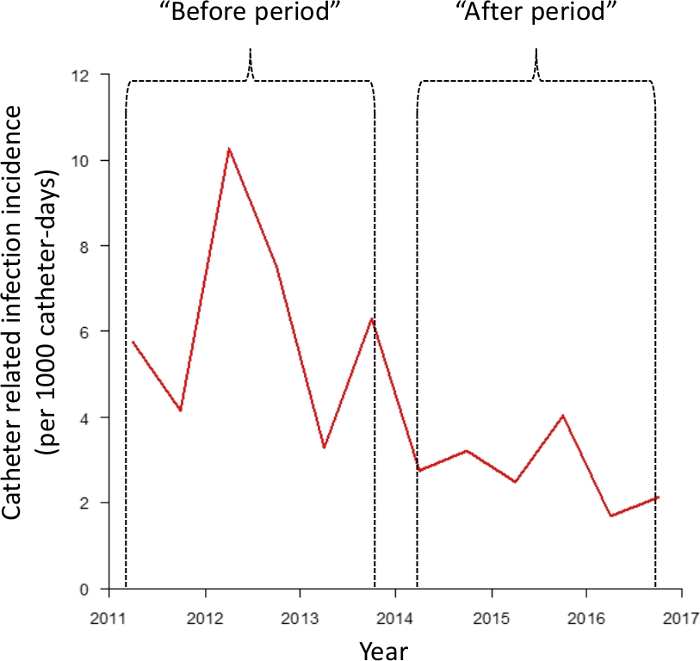
Figure 5: Evolution of catheter-related infection incidence before and after the use of connectors. Figure taken from Clavier et al.10 Please click here to view a larger version of this figure.
