Rabbits are widely used in animal experimentation due to their availability, high reproduction rate with short intergenerational times, and easy handling2. In our center, we use 5-7-day old New Zealand rabbits (Oryctolagus cuniculus) as a neonatal model to study the neurologic repercussions of extracorporeal surgery on the developing brain. As a result, we utilize procedures that require deep anesthesia and must use endotracheal intubation for periods of time up to an hour.
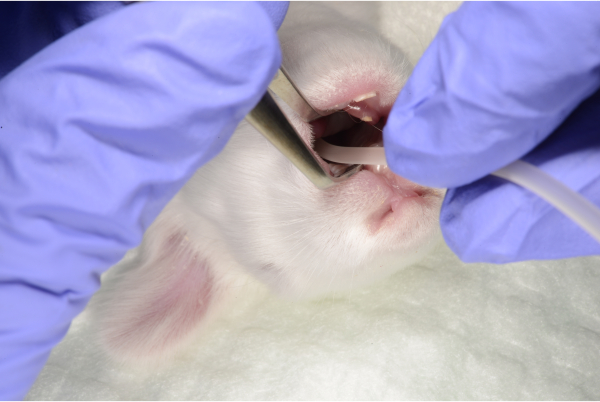
In the adult rabbit, several airway management techniques have been described, usually in a surgical context. When we tried to extrapolate these techniques to the rabbit kits, several problems arose. The rabbits weigh between 110 and 210 grams and have a maximum mouth opening range of 1 cm. These characteristics make direct visualization of the larynx difficult and it is complicated to find endoscopic material small enough. Another option described in the literature is to place an otoscope in the oral cavity and use it as a guide to introduce the PVC tube7. In newborn rabbits, both the presence of the tongue and the small size of the mouth make direct visualization of the glottis difficult. In addition, there are no supraglottic devices of adequate dimensions for newborns.
Due to the circumstances mentioned above, there are two fundamental mechanisms to secure the airway of the very small rabbit: tracheostomy and blind intubation. Tracheostomy is an invasive approach that has been used in both adult and newborn rabbits10, 12. It has the advantage of direct tracheal visualization, allowing the proceduralist to identify the exact location of the endotracheal tube. However, there is a high risk of mechanical complications and infection of the incision area, in addition to a decreased rate of survival of the animals once the procedures are completed13. Endoscopic/fiberoptic intubation is a method that would allow for direct visualization without surgery5. Another option to prevent laryngeal trauma is the use of a tight-fitting face mask, which has some additional drawbacks such as suboptimal ventilation and gastric distension.
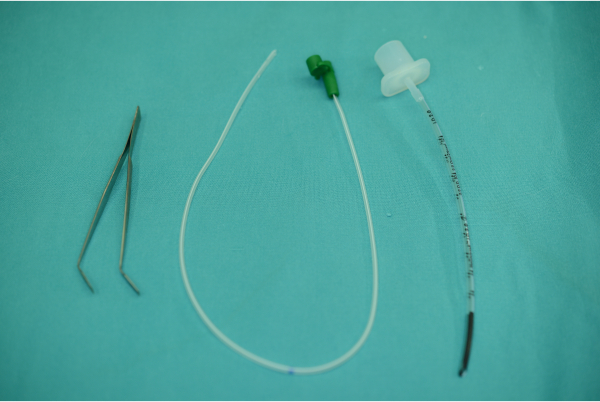
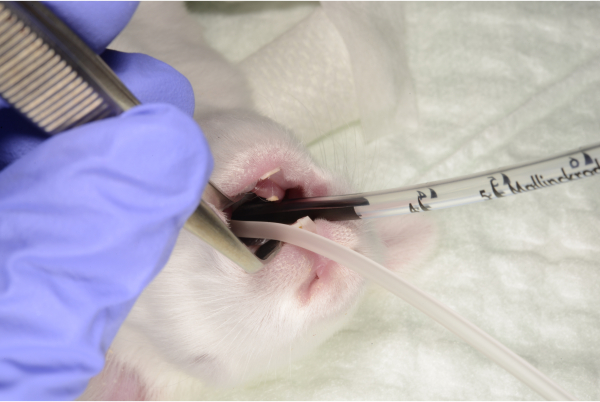
In the laboratory, blind intubation is used to manage newborn rabbit airways. This method has been described in the adult rabbit as a feasible technique with high success index6. In the initial experiments, we tried to perform this technique without occlusion of the digestive tract. The result was a high rate of introduction of the endotracheal tube into the esophagus. With the insertion of the gastric tube prior to intubation, however, successful intubation was achieved in 90% of cases. Regarding the size of the endotracheal tube, we initially tried to use peripheral venous catheters up to 14 gauge in diameter, observing difficulties in both insertion (greater rigidity) and ventilation (diameter too small and difficulty connecting to the ventilator). In our experience, the use of 2 mm internal diameter endotracheal tubes introduced to a depth no more than 3 cm has been the most effective in ventilating small rabbits, shown by correct gasometric and ETCO2 values. While intubation in adult rabbits generally requires hyperextension of the head to essentially a 90° angle to the horizontal surface of the table, we were able to perform the procedure with only a mild head extension.
One of the important elements to be considered when performing this procedure is the friable nature of the newborn rabbit trachea. Keeping this is mind, we introduce the pre-lubricated tube slowly and carefully to avoid tracheal perforation. We recommend not inserting the tube further than 3 cm, as this was found to be the optimal length during practice attempts, and halting the intubation if the proceduralist encounters any resistance; in this situation, it is preferable to remove the tube and start over. We experienced one case of likely tracheal perforation in the smallest animal in the cohort.
The main limitation of this technique is the difficulty in detecting the correct position of the endotracheal tube once introduced. In our experience, the advancement of the device without resistance, the detection of appropriate ETCO2, the fogging of the tube and visualization of thoracic expansion during ventilation, as well as the maintenance of vital signs have been sufficient to corroborate the suitability of the procedure in all cases. In some of the experimental subjects, arterial gasometries were performed during ventilation showing adequate levels of carbon dioxide and oxygen concentration. In addition, though histopathology analysis was not performed, previously published literature has described mucosal injury to the trachea in the absence of clinical changes secondary to intubation14.
In conclusion, the model of intubation in newborn rabbits we have described is a rapid technique that uses basic supplies and allows for effective ventilation. We believe this technique can be incorporated in the armamentarium of airway management of neonatal rabbits.