A total of 31 animals were included in the laboratory setting: 27 rats were included in the final statistical analysis; 4 rats died prematurely (12.9% mortality rate). Intraoperatively, breath distension was significantly (p = 0.03) reduced in stent- (12.9 μm ± 0.7) compared to coil-treated (13.5 μm ± 0.6) rats. Fluorescence angiography was performed for every rat at the end of the final FU. Reperfusion was indicated in all 6 coil-treated animals, whereas reperfusion was observed in only 12.5% of the 8 stent-treated animals.
Pooled baseline aneurysm volumes for day 7 and day 21 did not differ significantly (neither for decellularized (p = 0.9) nor vital (p = 0.1) aneurysms) between the coil- or stent-treatment groups (Figure 3). Pooled FU volumes for decellularized aneurysms showed a nonsignificant aneurysm growth in coiled compared to the stented aneurysms (p = 0.28), significantly greater in the vital coiled than the stented group (60.1 mm3 ± 31.1 mm3 vs. 20.5 mm3 ± 20.6 mm3; p = 0.002).
Amounts of cell-tracer-positive cells in the neointima of decellularized aneurysms did not significantly differ between the stent- or coil-treated groups at day 7 FU (p = 0.8) but were significantly higher in stented rats at day 21 FU (Figure 4; p = 0.04). In vital aneurysm-sutured rats, no significant differences were noted at either 7 days (p = 1.0) or 21 days (Figure 5) FU (p = 0.66). In decellularized aneurysms at 7 days FU, significantly more cell-tracer-positive cells remained in the thrombus of the stent-treated compared to the coil-treated group (p = 0.01). This difference was not observed in vital aneurysms at 7 days FU. See Table 1 for the proportion of cell-tracer-positive cells for decellularized, as well as vital coiled and stented aneurysms for day 7 and day 21 FU. Counterstaining for von Willebrand factor (F8) was performed in the endothelial cells of the neointima of each rat (Figure 6).
The average duration of the surgical procedure was 119.1 ± 21.3 min for the coiling group compared to 154.1 ± 30.2 min for the stent group (p = 0.001). The number of stitches for aneurysm sutures also differed significantly (p = 0.000002) for the coil (15.6 ± 2.9 stitches) and stent groups (11.3 ± 1.1).
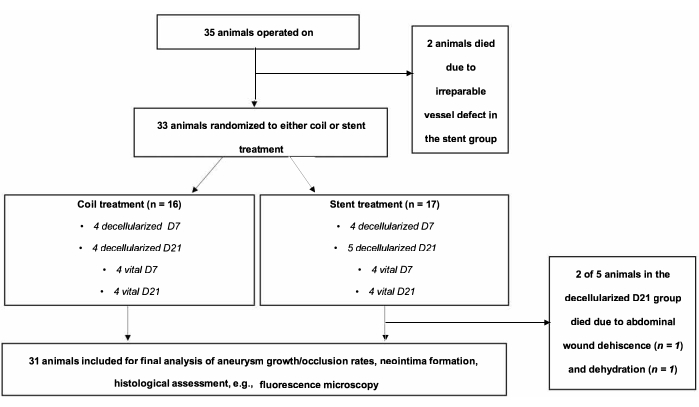
Figure 1: Flow chart of the experimental setting. A total of 35 animals were operated on and randomized to coiling or stenting groups. Two animals of the stent group died in the immediate postoperative course. Please click here to view a larger version of this figure.
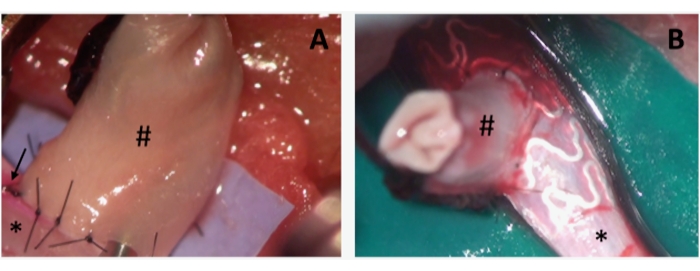
Figure 2: Intraoperative photographs of aneurysms during coil and stent embolization. (A) depicts a sidewall-aneurysm (#), sutured on the abdominal rat aorta (*). Note the coil device introduced in the aneurysm before performing the last single stitch to complete the aneurysm suture. Note the pinkish staining (arrow) on the left side of the arteriotomy, indicating the correct distribution of the cell tracer. (B) The same setting as in A, showing the stent device already in situ. Please click here to view a larger version of this figure.
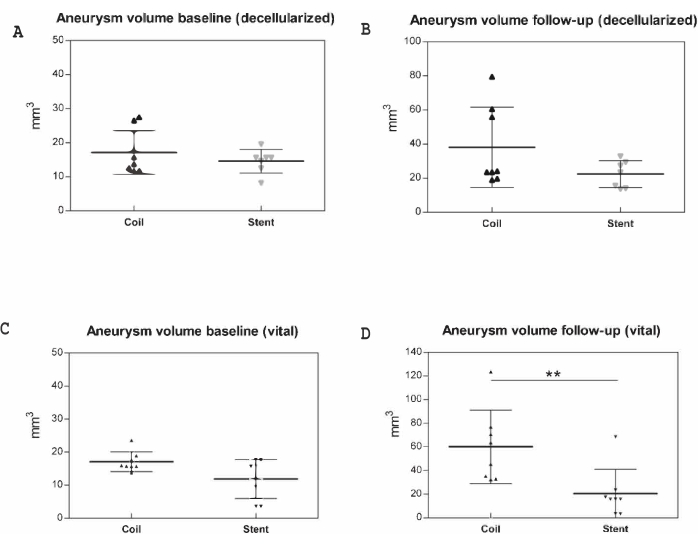
Figure 3: Macroscopic postmortem measurements in 31 animals. Aneurysm volumes (mm3) were documented prior to implantation and at follow-up, represented along the y-axis. (A) Baseline (decellularized), (B) follow-up (decellularized), (C) baseline (vital), (D) follow-up (vital). Data for day 7 and day 21 are pooled. ** p < 0.01. Values are expressed as medians with interquartile ranges. Please click here to view a larger version of this figure.
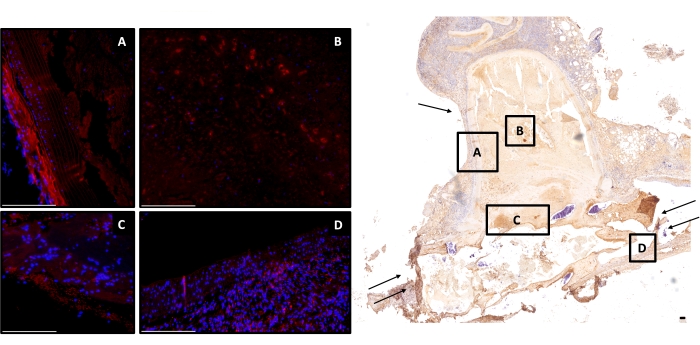
Figure 4: Exemplary image of a stent-treated decellularized aneurysm at day 21. Right, image overview of a monoclonal antiα-SMA, cell-depleted aneurysm (2-fold magnification) is shown; scale bar = 150 μm. Left, counterstained with DAPI; red cells are cell-tracer-positive (A) in the aneurysm wall, (B) in the thrombus, (C) residual stained but faded cell-tracer-positive cells in the neointima, and (D) in the adjacent vessel complex. Scale bars = 100 μm (A–D). Single arrow marks the aneurysm wall, double arrow the parent artery. Abbreviations: DAPI = 4',6-diamidino-2-phenylindole; α-SMA = α-smooth muscle actin. Please click here to view a larger version of this figure.
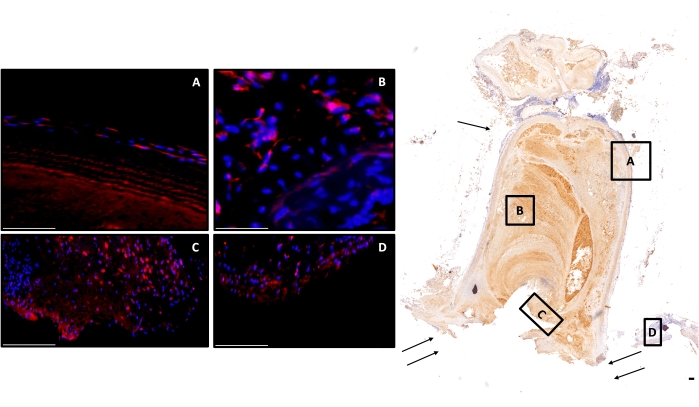
Figure 5: Exemplary image of a coil-treated vital aneurysm at day 21. Right side, image overview of a monoclonal antiα-SMA, cell-rich aneurysm (2-fold magnification) is shown; scale bar = 150 μm. Left side, counterstained with DAPI; red cells are cell-tracer-positive (A) in the aneurysm wall, (B) in the thrombus, (C) multiple positive cells in the neointima, and (D) in the adjacent vessel complex. Scale bars = 100 μm (A–D). Single arrow marks the aneurysm wall, double arrow the parent artery. Abbreviations: DAPI = 4',6-diamidino-2-phenylindole; α-SMA = α-smooth muscle actin. Please click here to view a larger version of this figure.
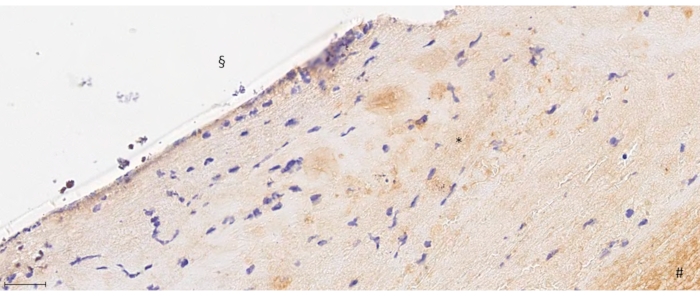
Figure 6: 40-fold magnification from F8 staining. # depicts the thrombus formation, * the neointima, and § the endoluminal side below the aneurysm orifice. Note the endothelial layering shown as purple staining in the endoluminal layer of the neointima. Scale bar = 175 μm. Please click here to view a larger version of this figure.
| DAPI/CM-Dil dye (%) | Coil | Stent | |||
| Day 7 | Day 21 | Day 7 | Day 21 | ||
| Decellularized pouches | Neointima | 68.00% | 7.70% | 72.20% | 34.30% |
| Parent artery | 75.50% | 10.50% | 76.50% | 35.60% | |
| Thrombus | 7.50% | 5.50% | 25.20% | 8.30% | |
| Aneurysm wall | 12.20% | 8.50% | 11.70% | 9% | |
| Vital pouches | Neointima | 56.70% | 11.50% | 58.20% | 15.00% |
| Parent artery | 60.00% | 24.20% | 81.50% | 26.00% | |
| Thrombus | 62.00% | 26.20% | 71.20% | 23.70% | |
| Aneurysm wall | 13.20% | 10.20% | 13.50% | 11.60% |
Table 1: Proportion of cell-tracer positive cells in neointima, parent artery, thrombus, and aneurysm wall. Values are depicted as percentages for decellularized and vital pouches for coil and stent treatment for day 7 and day 21. Abbreviation: DAPI = 4',6-diamidino-2-phenylindole.
Video 1: Cell-tracer injection in the abdominal part of the rat aorta. This technique is performed using a one-point injection into the clamped rat aorta. Please click here to download this Video.
