Epidemiological data indicates that worldwide there are ~17 million new cases of stroke each year, with an increase in incidence in low- and middle-income countries1. The number of new cases is estimated to increase to 77 million by 20302. Motor impairment due to stroke often affects patient's mobility and participation in daily life activities, contributing to a low quality of life. Traditional motor rehabilitation includes manual therapy, but over the past few decades, robotic systems for rehabilitation have been developed. These systems can deliver therapy at high intensity, dose, quantifiability, reliability, repeatability, and flexibility3 and have shown potential as effective rehabilitation treatments for both acute and chronic stroke patients4,5,6. In addition to delivering therapy, robotic systems for rehabilitation can be used as evaluation tools as they can be equipped with sensors that can measure patient movement kinematic/kinetic data7,8. For upper extremity motor rehabilitation, such data has not only been proven to be useful for assessing the level of patient's motor recovery elicited by robotic therapy and served as a supplementary tool to traditional clinical assessments9,10, but it has also contributed to advancing the understanding of the process of motor recovery from stroke11,12 as well as neural control of movement and motor learning in healthy subjects3,13,14. As a result, these findings have provided a foundation for enhancing rehabilitation treatments15.
Over the last two decades, many robotic devices for lower limb neurorehabilitation have been proposed, spanning from exoskeletons that support the patient body weight during walking (e.g., over a treadmill, such as Lokomat16) to stationary robotic systems that allow the patient to exercise the ankle, knee or foot without walking (such as the Rutgers Ankle17, the High-Performance Ankle Rehabilitation Robot18, and the Gwangju Institute of Science and Technology (GIST) ankle/foot rehabilitation robot19) or active foot orthoses that are actuated exoskeletons worn by the patient to walk overground or over a treadmill (such as the Powered Gait Orthosis20 and the MIT Anklebot21). See22,23,4 for a review on robots for lower limb rehabilitation.
Results of clinical studies of robotic devices for lower limb rehabilitation on stroke patients have been encouraging and have shown that these systems may improve joints' Range of Motion (ROM), muscle strength, or gait, depending on the specific device and clinical protocol (see 24,25 for a review on the efficacy of lower limb robots for rehabilitation). While it has been postulated that robot-assisted therapy promotes neuroplastic changes, which ultimately result in improved motor abilities26, how the process of motor recovery from stroke exactly occurs and which robotic training protocols optimize the process of recovery of lower limb motor abilities, remain mostly unclear. In fact, there is a significant, growing disparity between the increasing development of rehabilitation robots (either by academic researchers or commercial entities) and the limited understanding of the neurophysiological mechanisms that underlie motor recovery4. Measurements of movement kinematics or joint torques taken with embedded sensors have contributed to quantitatively describing motor behavioral changes that occur as patients recover lower limb motor abilities27,28,29, partially filling this gap. However, the neural correlates underlying such changes have been less investigated. This is due to several reasons.
Brain functional imaging is time-consuming and sometimes difficult to complete in the context of clinical trials, which often require keeping patient burden minimal to maximize the likelihood of patient adherence to the study. This holds particularly true for individuals who have suffered a stroke, given the fact that post-stroke fatigue and muscle weakness are frequently observed30. Also, imaging modalities that are based on magnetic fields, such as functional Magnetic Resonance Imaging (fMRI), require both patient and robotic hardware to be magnet-safe.
Among non-invasive imaging modalities, functional Near-Infrared Spectroscopy (fNIRS) is an imaging technique particularly suitable for assessing areas of brain activation in subjects undergoing robotic therapy. Similarly to fMRI, fNIRS measures blood oxygenation/deoxygenation in the brain. However, unlike fMRI, fNIRS is fully compatible with robotic hardware, and it is often portable, even being usable at the bedside. Also, fNIRS has low cost and less sensitivity to motion artifacts31,32,33.
Despite its clear advantages and widespread use in many clinical settings since its first introduction in the late 70s34, only a few studies have used fNIRS to quantify brain activation associated with lower limb movements and stroke motor recovery. FNIRS studies aimed at elucidating mechanisms of neural control of movement and/or mechanisms or evaluation of motor recovery from stroke have mostly investigated single-joint movements (e.g., dorsiflexion, plantar flexion or knee extension movements35,36,37), walking38,39,40,41,42,43, or cycling44. See45 for a review. Similarly, fNIRS studies on robot-assisted therapy for the lower limb have mostly focused on robot-assisted gait rehabilitation; see46 for a review. A few studies have focused on using fNIRS as part of a Brain-Computer Interface (BCI) system to derive control signals for robotic devices47,48; while this research area also relies on the processing of fNIRS signals, its goal is different and mainly focused on decoding patient intentions (e.g., patients with severe motor disabilities).
The pilot study presented herein is part of an initial effort to investigate the effects of a robotic system for lower limb rehabilitation. The robot can deliver target-oriented lower limb rehabilitation that involves training in everyday multi-joint movements as well as deliver therapy to single joints (e.g., knee or ankle) of the lower limb (i.e., implement a bottom-up rehabilitation program).
The study aimed to investigate the feasibility of an experimental protocol that required the acquisition of fNIRS data during the performance of lower limb, multi-joint pointing movements. The duration of the data acquisition period in this study, which was limited to 6 min, is shorter than typical fNIRS protocols. This was a deliberate choice made with the aim of enhancing the practicality and clinical applicability of this research, particularly in patients with limited mobility or strength. Identifying fNIRS correlates of such complex multi-joint movements and gaining insights into how brain activation was modulated by robot assistance were also points of interest. For this purpose, two sessions of experiments were conducted with the same participants: one with no robot assistance and one with robot assistance. Finally, it is important to remark that this study focused on healthy subjects in order to establish a foundation for future research in terms of recording protocol feasibility and evaluation of brain activation during movements targeted by robotic therapy.
Apparatus
A portable robot designed to deliver lower limb rehabilitation (see Figure 1) was used to conduct our experiments. The robot has a 3D reachable workspace and is compact and light, weighing about 35 lb., which makes it easy to transport and install.
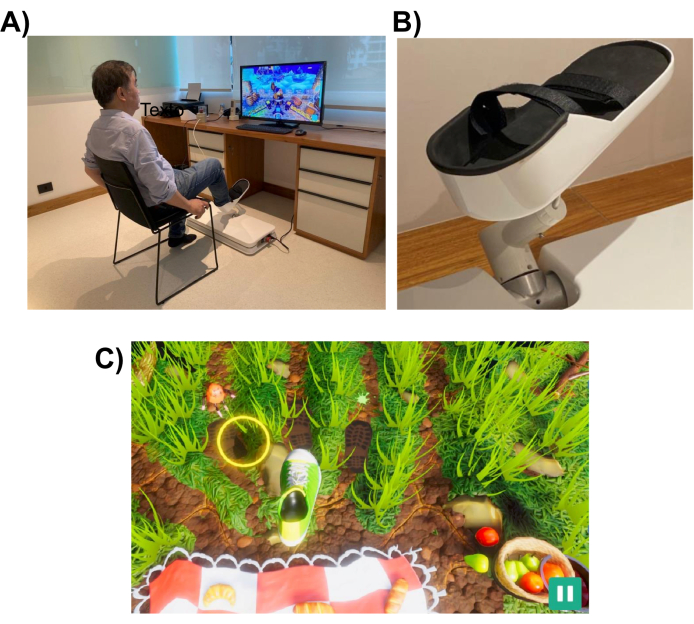
Figure 1: Experimental setup. (A) The robotic system (installed on the floor) designed for the lower limb. A volunteer is shown utilizing the interface with their right foot. (B) Support structure for the subject's foot that enables attachment to the robotic system. (C) A screenshot of the Picnic game. The objective of the game is to move the foot (green and white shoe) to the target (yellow circle). Please click here to view a larger version of this figure.
The robotic system is designed to assist a patient in performing lower limb movements similar to those performed in everyday tasks, such as pointing or kicking. It uses interactive virtual reality games, which are displayed on a computer monitor or a television screen placed in front of the robotic device (see Figure 1). The robot-end effector is attached to the patient's lower limb (e.g., ankle), and its position is mapped to the position of a cursor on the screen. A typical game shows the patient movement targets (e.g., the object to point to or where to kick the ball).
To complete the movement task, the robot may assist the patient with a level of assistance that can range from full assistance to none. The level of robotic assistance is chosen at the beginning of each rehabilitation session based on the patient's level of motor impairment. The movements performed by the subject are used by the game to score the patient's performance and provide them feedback on their performance (e.g., ROM, number of movements, and level of robotic assistance). The games are designed to be interactive and entertaining to sustain patient interest and attention. In this study, participants played the "Picnic game", in which the player had to stop the insects from reaching the towel and stealing the food (see Figure 1, bottom panel, for a screenshot).
Data acquisition was performed with a portable fNIRS acquisition system with two different continuous-wave optodes (760 nm and 850 nm), 8 dual-tip LED sources, and 8 dual-tip active detectors. The signals were acquired using a sampling rate of 10.17 Hz. A laptop was used for the calibration optimization and signal recording using a Wi-Fi network created by the fNIRS system.
A cap was used to hold the optodes in the predetermined locations. The sources and detectors were placed according to the 10-10 international EEG system in a grid spatial distribution. Each fNIRS channel was defined by a source-detector pair with inter-optode distances of approximately 30 mm. The optodes were placed over the supplementary motor, premotor, and motor areas at the locations shown in Figure 2. The total number of channels was 28, where 8 were short-distance channels that were coupled to each source using a fiber optics adapter to a single detector. Given the multiplexing setup of the hardware, it is possible to acquire short-distance information from all sources using only one detector.
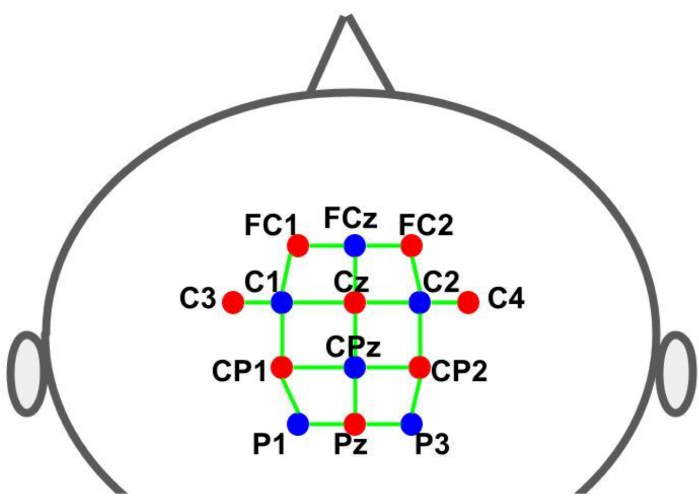
Figure 2: Montage layout using the 10-10 EEG system. The letters and numbers indicate the source/detector locations. The red and blue dots represent the source and detector optodes, respectively. The green lines represent the fNIRS channels which consist of source and detector pairs. Please click here to view a larger version of this figure.
Experimental design
The experiment was conducted under two distinct experimental conditions, differing in the level of assistance provided by the robot for the subject's movements. In the first condition, the robot was programmed not to provide any assistance to the subject's movements, while in the second condition, the robot controlled the subject's foot and leg movements (robot-assisted movement).
Each experiment followed a block design paradigm involving alternating cycles of a motor task (playing the game – 30 s) and resting (30 s), as illustrated in Figure 3. The starting and conclusion of each phase (play/game or rest) were visually signaled to the subject through the computer screen. During the rest phase, a message indicating a pause was displayed. Each cycle (play/game + rest) had a duration of 60 s and was repeated six times, resulting in a total runtime of 360 s (6 min).
The participants played the "Picnic game", wherein the objective was to prevent insects from reaching the towel and stealing food. This game involved a sequence of lower limb movements, starting from a designated home target (initial position) and extending towards one of three outer targets before returning to the home target. On the screen, the outer targets were visually represented as animated moving insects, which the participants had to reach and step onto. There were three outer-reaching targets, each randomly presented an equal number of times, alongside a common home target for every movement. The distance that the foot needed to travel from the home target to the position of the outer targets formed an arc, approximately measuring 26 cm. The motor task required the execution of multi-joint movements, demanding coordination between knee flexion/extension, plantar flexion, and dorsiflexion movements.
The fNIRS data recordings were synchronized with the visual stimuli presented by the game to the subject through a transistor-transistor-logic (TTL) pulse generated by the robot. Pulses were generated at the outset of each phase (play/game and rest). Thus, all timing control was performed by the game, which provided visual cues (targets) to the participant to start each movement, sent TTL signals to the fNIRS system to mark the brain activity recordings, and, if required by the experiment, sent signals to the robot control system to initiate movement assistance.
All six subjects completed both experiments. In the no-assistance condition, an average of 76.67 trials (std. 10.73) was completed by each subject (note, for each subject, the number of trials depended on the number of successful reaches since a new target was only shown if the previous one was reached). In the assistance condition, where the subject's movement was fully aided by the robot, all subjects completed 70 trials. fNIRS data was successfully recorded from all subjects.
Figure 4 shows the single-subject brain activation maps comparing the play/game vs rest periods for HbO and HbR. For each subject, the maps associated with HbO changes showed statistically significant activation (p < 0.01) in the experimental condition with no robot assistance, while only two subjects showed statistically significant activation in the experimental condition with robot assistance. Regarding HbR, four subjects presented statistically significant activation (p < 0.01) in both conditions, albeit in fewer channels as compared to HbO.
Figure 5 summarizes the individual subjects' results of the ROI-based hypothesis-driven analyses. Among all ROIs examined, only the left premotor cortex displayed a statistically significant increase in HbO activation during the game/play relative to rest comparison (p = 0.046) and only in the condition without robotic assistance. In addition, this ROI presented a greater activation in the condition without robotic assistance in comparison to the condition with robotic assistance (p = 0.016). There were no statistically significant differences for the other ROIs or in HbR-based analyses, either in play/game vs. rest analyses or in comparisons between conditions (p>0.05). Thus, at the group level, no statistically significant differences were found at the left somatomotor cortex, SMA, or in HbR-based analyses.
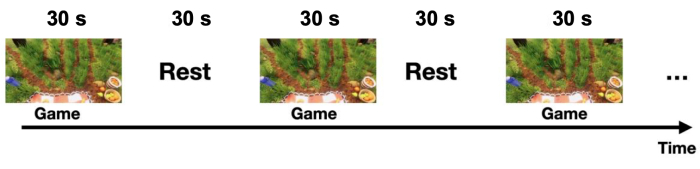
Figure 3: Block design experiment with alternated blocks of game and resting state conditions. The subject played the Picnic game continuously for 30 s (game period) and remained still for the following 30 s (rest period). This cycle was repeated 6 times, resulting in a session duration of 6 min (note, only 150 s are shown in the figure). Please click here to view a larger version of this figure.
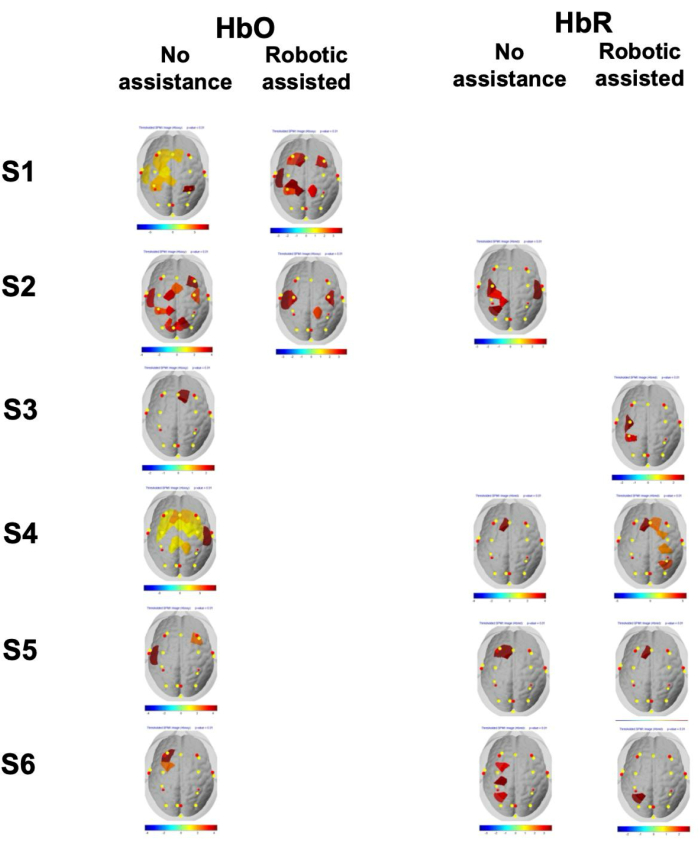
Figure 4: Single-subject brain thresholded statistical activation maps. Single-subject brain thresholded (channel p-value < 0.01) statistical activation maps of the six subjects (S1-S6) for HbO and HbR in both experimental conditions (movements with and without robotic assistance). Note that only maps displaying a statistically significant activation are presented (i.e., any subject and condition with a blank slot indicates that no significant activation was observed for that particular combination). The color bar represents the t-statistics amplitude of the activation coefficient (GLM beta) of each fNIRS channel. Please click here to view a larger version of this figure.
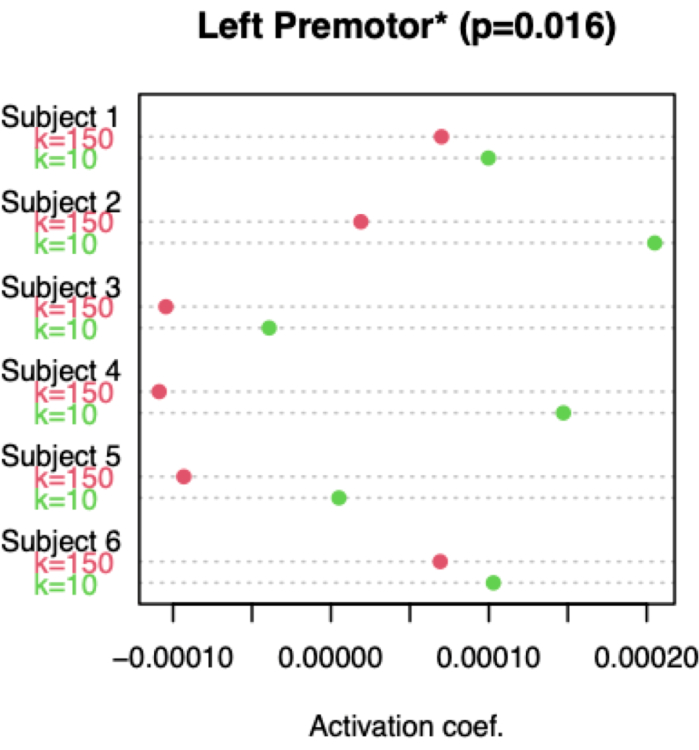
Figure 5: Activation of left premotor cortex based on HbO signals. As detailed in step 5.2, the beta coefficients were estimated using a GLM, and the amplitude of activation was quantified for each subject, experimental condition (unassisted and assisted movements), and specific channels (note, the beta values for the ROI were obtained by averaging the channels within the left premotor cortex). The dot chart visually represents the ROI average beta coefficients for each subject and condition, with the red and green dots indicating the assisted and unassisted movements, respectively. For each subject, the ROI beta coefficient of the unassisted condition is greater than that of the assisted condition, signifying greater activation in the former condition. This result is consistent across all subjects. Please click here to view a larger version of this figure.
