All of the results are in the context of 4 h of reperfusion following 12 h of NPV-ESLP16. During lung explant, there are several clinical outcomes to anticipate (Figure 3). Typically, the pig will remain hemodynamically stable following a successful left lung explantation but may require a low dose infusion of phenylephrine (dose range: 2-10 mg/h) due to a vasodilatory response to surgery. Heart rate should target approximately 100-120 bpm, respiratory rate (RR) 8-30 for SpO2 > 90%, mean arterial pressure (MAP) > 60 mmHg, normothermic (38 °C), and tidal volumes (TVs) are targeted at 5 mL/kg while on one-lung ventilation with peak pressures of 20-24 cm H2O. During one-lung ventilation, the ventilation volumes were reduced by half to protect the left lung from overinflation. The respiratory rate was increased to target a physiologic end-tidal carbon dioxide level (Figure 3). Thus, Figure 3 displays typical hemodynamic and ventilatory parameters during critical points of the transplant.
During lung implant, the following results are typical. The left lung will have absorbed fluid during the ESLP run and appears heavier and larger than the explanted lung. For this reason, the recipient should be slightly larger than the donor (2-4 kg), so the thorax can accommodate the somewhat edematous lung. The lung will require gentle pressure to insert into the chest through the thoracotomy. It is easier to insert the lower lobe first, followed by the upper lobe. The bronchus is a direct end-to-end anastomosis and should be performed first. 4-0 prolene on a TF needle is recommended. The LA cuffs are highly friable but not too difficult to sew due to the redundancy and pliability of the tissue. 6-0 prolene on BV-1 needles work well for the LA anastomoses. The PA is the last anastomosis performed. This vessel can tear easily with little traction. If it tears, it is possible to open the pericardium and move the clamp proximally toward healthy tissue for sewing. Again, a 6-0 prolene on BV-1 needles works well for this anastomosis.
At the time of reperfusion, the following trends were noticed. Once the bronchus is unclamped and TVs are increased back to 10 mL/kg, the left lung will begin to inflate. Although the target was 10 mL/kg for tidal volumes, generally 6-8 mL/kg was attained, which is achieved gradually over the first 2-3 h of reperfusion, depending on the ESLP protocol used and the quality of the implanted lung. Rarely, there can be a small air leak, and this can be remedied with a simple stitch on the anterior wall. The posterior wall is more difficult to repair and will require packing. Great effort should be made to avoid air leaks from the bronchial anastomosis. Upon bronchoscopy, the right lung appears normal, and the left lung is typically edematous. The suture line is inspected, and approximately 50-100 mL of clear fluid is suctioned from the airways. The TV will drop significantly during suctioning from 300 s to 20 s, so this action should be performed quickly to allow the pig to recover. If arterial saturation drops below 90%, the bronchoscopy should be terminated, and the pig is allowed to recover over 1-2 min of ventilation. The first arterial blood gas (ABG) is typically normal because the right lung is functioning well as the left lung recovers.
The proactive administration of furosemide, dextrose, and insulin at the time of reperfusion serves to mitigate a dramatic rise in potassium through intracellular shifting. The potassium will predictably rise during 60-120 min of reperfusion (Table 1). Table 1 demonstrates a sample of ABGs over transplantation with 4 h reperfusion following 12 h of normothermic negative pressure ventilation (NPV) ESLP. Approximately two to four shifts are required during 4 h reperfusion to keep potassium < 5 mmol/L. If the trend is upward and appears as a rapid change between two gases drawn at 30 min intervals, the target is K+< 4.5 mmol/L. Shifts include 40 mg of furosemide, 100 mL of 25% dextrose (D25), and 10 units of regular insulin administered as IV push via the central line. Occasionally, the pig will require a low dose dobutamine infusion (1.5-5 mcg/kg/min) along with phenylephrine (2-10 mg/h) after 30-60 min of reperfusion to treat a developing vasoplegic response. It is preferable to use phenylephrine in this situation exclusively. However, dobutamine can be a useful supplemental inotrope to maintain a mean arterial pressure greater than 60 mmHg, particularly if the heart rate is bradycardic.
Upon thoracotomy closure and turning the pig prone, an improvement in ventilation and hemodynamics is demonstrated. The modification can be drastic and occur over 5-10 min, but occasionally the response takes 1 h. Tidal volumes increase as pressure/weight is taken off the right lung, and the left lung continues to ventilate with improved compliance and recruitment. A repeat bronchoscopy can be performed further to clear the airway after a change in position. Over the following 4 h, phenylephrine requirements decrease, TVs approach the target 10 mL/kg, and ABGs stabilize (Table 1). To reiterate, if TVs of 10 mL/kg are targetted, typically TVs in the range of 6-8 mL/kg are achieved (Figure 3).
At the time of the final isolated left lung assessment, a stable pattern of behavior has been observed. The pig is less tolerant hemodynamically in the supine position for sternotomy and may require additional vasopressor support. Inspection of the left lung reveals variable degrees of mild hyperemia from ischemic reperfusion injury (IRI). The right lung appears normal. Upon clamping the right hilum, the pig becomes sinus tachycardic (120-140 bpm), and 100% of the cardiac output is diverted to the left lung. Targeted tidal volumes are not decreased at this time as the entire process takes 10 min. The pig remains stable up to the 5 min mark, but the heart may develop ventricular fibrillation between 5-10 min and manual cardiac massage is potentially required to continue perfusing the left lung. The left lung is explanted, weighed, and the anastomoses are inspected for patency. The pig expires rapidly at the time of exsanguination, which coincides with the explantation of the previously transplanted lung.
A successful transplant has predictable findings after the experiment (Table 1 and Figure 4). Figure 4 displays typical P:F ratio changes and edema formation during the transplant protocol. Typically, the left lung will experience an approximate 35% (+/-15%) weight gain; however, residual blood in the circulation contributes to this weight. PF ratios drop by approximately 100 at reperfusion as the left lung is not immediately effective at oxygenation, but this discrepancy improves over 2-3 h. Upon isolated left lung assessment at 4 h, the PF ratio will remain stable or decline slightly. Generally, the isolated left lung gas at 10 min will be similar to the final gas analysis post 12 h ESLP (Table 1). However, this is entirely dependent on the ESLP protocol employed, and the extent of IRI incurred. An unsuccessful transplant can be caused by clotting of the LPA, which results in an infarcted lung that does not oxygenate. Likewise, the duration of the transplant surgery can affect the quality of the reperfused lung function. An implantation surgery should take between 30-60 min. Longer operations expose the donor lung to damaging warm ischemic time that exacerbates ischemic reperfusion injury and can confound the results of the experimental ESLP protocol. The specific ESLP protocol of a given experiment may produce a non-functioning lung that fails to oxygenate after transplantation despite patent anastomoses. Such isolated left lung gases will be very dark in color (deoxygenated) with a low partial pressure of oxygen (PaO2).
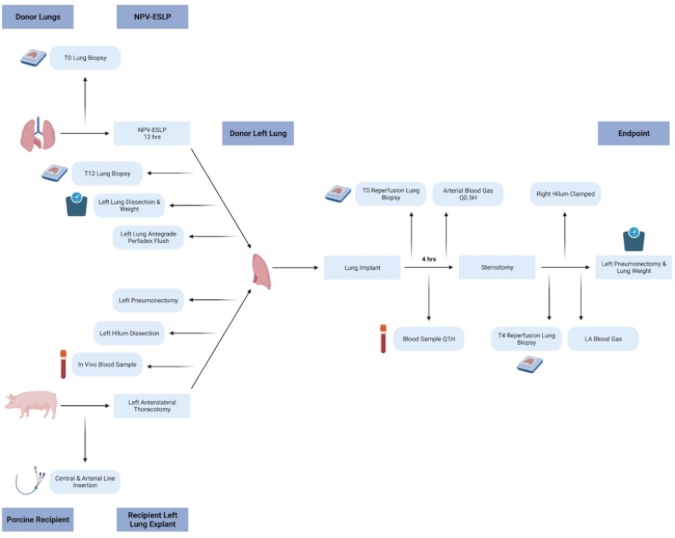
Figure 1: Schematic of porcine left lung transplant protocol. Schematic representation of 12 h NPV-ESLP run followed by left lung transplantation in a Yorkshire pig. Please click here to view a larger version of this figure.
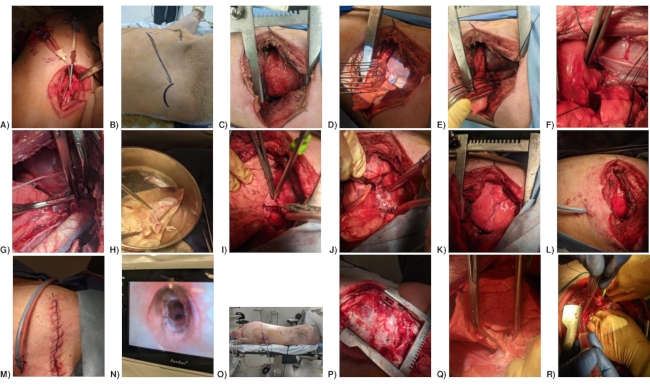
Figure 2: Photos of porcine left lung transplant surgery protocol. (A) Internal jugular and common carotid line placement. (B) Thoracotomy incision. (C) Thoracotomy. (D) Left Hemi-azygous vein. (E) Ligated Left Hemi-azygous vein. (F) Isolation of pulmonary veins. (G) Clamped left atrial cuff, left bronchus, and left pulmonary artery. (H) Left donor lung with pulmonary vein, bronchial and PA cuffs. (I) Pulmonary artery anastomosis. (J) Left lung transplanted and unclamped. (K) Lung repositioned. (L) Chest tube positioned. (M) Thoracotomy closure. (N) Bronchial anastomosis. (O) Pig in prone position. (P) Sternotomy. (Q) Accessory lobe clamped (Right lung clamped, but not shown). (R) Left pulmonary vein blood samples were drawn from pulmonary vein anastomosis (bleeding from prior puncture site). Please click here to view a larger version of this figure.

Figure 3: Monitoring and ventilation parameters for porcine left lung transplant surgery. (A) Typical parameters for recipient pre-transplant. (B) Typical parameters at recipient left lung explant. (C) Typical parameters 4 h post left lung donor transplant. Please click here to view a larger version of this figure.
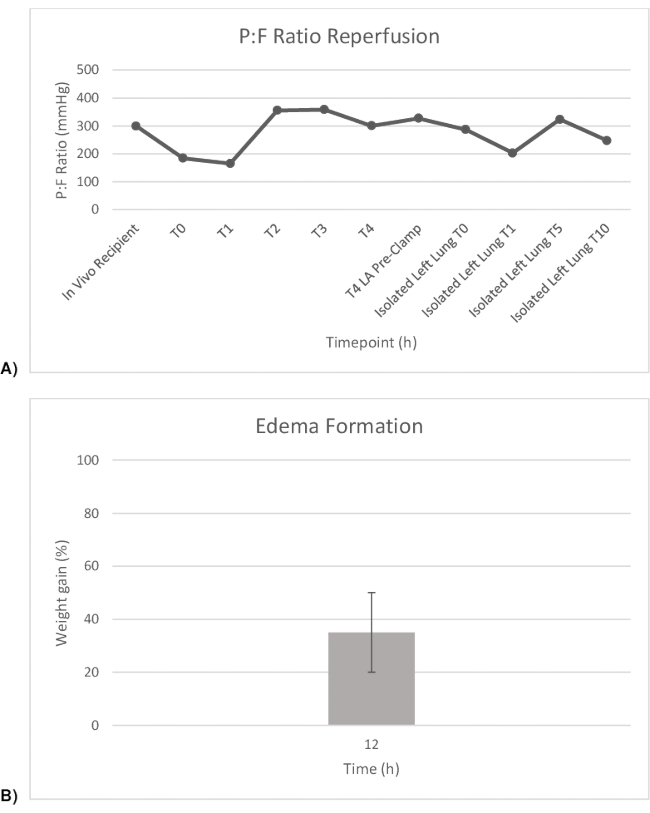
Figure 4: P:F ratio and weight gain pre-and post-transplant. (A) PaO2:FiO2 ratios throughout the transplant. (B) Weight gain of left lung throughout transplant after 12 h of NPV-ESLP. Please click here to view a larger version of this figure.
| Arterial Blood Gases (100% FiO2) | In vivo Recipient | T0 Reperfusion | T1 Reperfusion | T2 Reperfusion | T3 Reperfusion | T4 Reperfusion | Isolated Left Lung Pre-clamp | Isolated Left Lung Post-clamp (0 min) | Isolated Left Lung Post-clamp (1 min) | Isolated Left Lung Post-clamp (5 min) | Isolated Left Lung Post-clamp (10 min) |
| Blood Gas Values | |||||||||||
| pH | 7.402 | 7.327 | 7.284 | 7.402 | 7.421 | 7.479 | 7.504 | 7.399 | 7.371 | 7.423 | 7.435 |
| pCO2 (mmHg) | 47.7 | 57.3 | 56.4 | 36.9 | 35.3 | 35.6 | 34.2 | 45.6 | 48.1 | 40.6 | 36.6 |
| pO2 (mmHg) | 299 | 184 | 165 | 355 | 358 | 300 | 327 | 287 | 207 | 335 | 249 |
| Oximetry Values | |||||||||||
| Hb (g/dL) | 11.2 | 12.5 | 11.3 | 11.6 | 10.3 | – | 17.1 | 11.7 | 13.5 | 16.3 | 13.8 |
| sO2 (%) | 100.1 | 99.2 | 99 | 99.8 | 99.8 | – | 99.9 | 100.2 | 99.7 | 99.8 | 99.9 |
| Electrolyte Values | |||||||||||
| K+ (mmol/L) | 4.5 | 6.2 | 4.4 | 4 | 4.1 | 4.6 | 5.2 | 5.4 | 5.3 | 6.9 | 7.4 |
| Na+ (mmol/L) | 141 | 143 | 140 | 245 | 145 | 144 | 140 | 141 | 139 | 137 | 136 |
| Ca2+ (mmol/L) | 0.99 | 0.88 | 0.81 | 0.74 | 0.66 | 0.61 | 0.36 | 0.98 | 0.42 | 0.36 | 0.38 |
| Cl– (mmol/L) | 97 | 97 | 95 | 101 | 100 | 96 | 91 | 102 | 94 | 91 | 94 |
| Osm (mmol/kg) | 287 | 287.9 | 293.7 | 292.4 | 297.5 | 293.5 | 284.7 | 287.1 | 282.9 | 278.2 | 277.1 |
| Metabolite values | |||||||||||
| Glucose (mmol/L) | 4,2 | 2.7 | 13.4 | 2.8 | 8.3 | 5 | 5.1 | 4.9 | 4.5 | 4.6 | 4.2 |
| Lactate (mmol/L) | 1.2 | 1.3 | 3.8 | 2.5 | 1.3 | 1.2 | 1.4 | 1.8 | 1.4 | 1.9 | 2.7 |
| Acid Base status | |||||||||||
| HCO-3 (mmol/L) | 29 | 29.1 | 25.9 | 22.4 | 22.5 | 26.1 | 26.7 | 27.6 | 27.1 | 26.1 | 24.1 |
Table 1: Blood gas analysis performed following left lung transplant post 12 h of ESLP. Ca+, calcium ion; Cl–, chloride ion; Hb, hemoglobin; HCO3–, bicarbonate ion; K+, potassium ion; Na+, sodium ion; Osm, osmolarity; paCO2, arterial partial pressure of carbon dioxide; PaO2, arterial partial pressure of oxygen; sO2, oxygen saturation; isolated left lung pre-clamp, right hilum open; Isolated left lung post-clamp, 1 min after right hilum clamped.
Supplementary File 1: Surgical safety checklist for left lung transplantation. Please click here to download this File.
