All procedures were conducted under institutionally approved protocols with patient consent. See Figure 1 for an image of the intervention kit and main components and Figure 2 for the RS-tDCS session structure.
1. Pre-intervention procedures
- Perform recruitment pre-screening according to inclusion and exclusion criteria. Include patients who are adult amputees, who regularly experience phantom pain once a week or more with an intensity level of at least 4 on a Visual analog scale (VAS), and who do not have contra-indications to tDCS or unstable comorbidities.
NOTE: The sample size was calculated according to a calculation on our preliminary results from a previous RCT and our meta-analysis on tDCS effects, considering the minimally clinically significant difference of an effect size of 0.5 (80). We assumed a type I error of 5% and type 2 of 20% using a t-test calculation for differences and expanded to account for a 10% attrition rate. Reaching 145 subjects per group, 290 total. - Enroll the subject in the research study by filling out the registration, including the informed consent form, date of birth, gender, and questions about medical history and amputee profile.
- Perform the screening during the consent visit.
- Set up a date for the baseline and randomization process.
- Baseline visit and training
- Have the patients go through a series of questionnaires regarding pain, sleep, quality of life, cognition, and mental health.
- Randomize the subjects (according to their treatment expectancy) into two groups: either RS-tDCS of the M1 with somatosensory testing (intervention) or usual care (control group).
- Have the patients receive their training according to the randomization, so they can familiarize themselves with the provided materials and practice for the real-time remote supervised procedure.
- Conduct this step in person but do it remotely if the distance and the patient's literacy dictate this. In this case, perform the same described procedures using the same materials but explain how to operate the devices during a Zoom meeting.
- Train the patients from the usual care group in the use of the wearable HRV monitor and its corresponding App installed in a provided tablet, as well as the Zoom platform integrated into a laptop.
- Introduce the subjects to the password-protected laptop, where key features will be explained (including password, switching on/off, and USB webcam connection).
- Show the participants how to join the meeting through a personalized and secured call ID meeting and password via the Zoom platform. Have the participants practice with the researcher at least once.
- To guarantee activity success, ensure that the participants are able to trial a real-in-time session recording of HRV.
- Guide the patients on the correct placement of the HRV wearable device (in the middle of the sternum line).
- Once the sensors have been checked for placement, introduce the participants to the password-protected tablet. Show the participants how to pair the devices, change the record name, start, end the recording, and save it.
NOTE: Ensure that all these previous steps will be performed by the patient with researcher guidance once and then repeated without guidance to guarantee information retention.
- Stimulation group, RS-tDCS
- Show an instructional video and repeat this video content with the patient step-by-step.
- Show the tDCS device to the patient while placed on a mannequin head. Explain the various parts of this device, and give the patient a chance to correctly clip the SNAPpads to the SNAPstrap and into the device.
- Using a mirror, ask the patients to put the SNAPstrap on themselves, as it was on the mannequin's head, until they achieve a comfortable level and make sure the participant is correctly aligning the cathode and the anode as well as the back strap to ensure correct placement.
- Turn on the RS-tDCS device and show the steps to follow until stimulation, how to access the stimulation menu, enter the stimulation code, and what to do in case they need to abort a session.
- Finally, ask the participants to go over all the steps again, either practicing or verbally based on self-assessed competency. Go over the visiting schedule and explain the normal flow of every visit.
- To guarantee training success, fill out a comprehensive checklist covering all essential aspects of training (Table 1).
| 1) Computer |
| · REDCap |
| · Open surveys |
| · Filling and submitting forms |
| · Zoom Log in and out |
| 2) Heart rate monitor |
| · Heart rate monitor app |
| · Correct placement |
| · Recording of the heart rate |
| 3) Home-Based tDCS |
| · Head and electrode preparation |
| · Gather the materials: sponges, head strap, the stimulator device, the saline solution, syringes, and the laptop provided by the Lab. |
| · Find the stimulation area (the central line of your head and your ear) – identified correctly the M1. |
| · Check the skin for redness or any sign of damage. |
| · Open the pre-soaked sponges and attach the electrodes (located inside the pre-soaked sponges) to the head strap. |
| · If the sponges are not wet enough, prepare with the correct amount of saline solution (approx. 6ml on each side). |
| · The sponge in the M1 area. |
| 4) Device preparation and Stimulation |
| · Connect the electrode cable to the tDCS device, according to the matched colors (red cable into the red entrance and the black cable into the black entrance). |
| · Before starting, turn on the computer and open the conference call. |
| · Follow the instructions provided by the research team. |
| · Turn on the device. |
| · Press any button to get the main menu screen. |
| · Press the button to start stimulation. |
| · Check the quality of the setup ( If the quality is not good, tell the team and wait for instructions). |
| · Press the pound button and correctly enter the activation code to start the stimulation. |
Table 1: Training checklist.
2. Study intervention visits
NOTE: The study consists of a total of 23 visits, with 20 sessions involving either stimulation or usual care. Throughout the intervention part, regardless of group allocation, both will be connected to the trained researcher staff via Zoom.
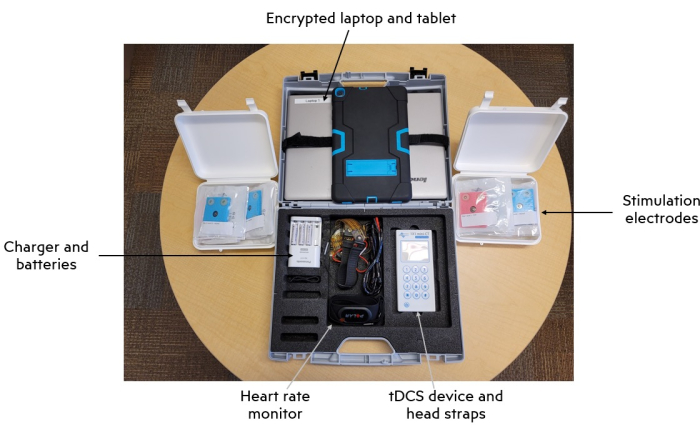
Figure 1: Intervention kit and main components. Abbreviation: tDCS = transcranial direct current stimulation. Please click here to view a larger version of this figure.
- When the patients are at home, connected via Zoom meeting, begin the session by asking the patient about their levels of PLP, phantom limb sensations (PLS), residual limb pain (RLP), and telescoping experienced within the past 24 h by using the VAS score, which is the primary outcome.
- Have the patient begin recording their HRV (measured for the secondary outcome).
- Ensure the correct positioning of the device (middle of the sternum line), as well as its pairing with the tablet to guarantee accurate recordings.
- Remind the patients at the beginning of each session about their research ID and the visit number.
- Have the patients show the tablet screen through the webcam to ensure the recording is being performed accordingly.
- After 5 min, have the patient stop and save the recording by the patient in the App. When questions arise, guide the patients throughout by remaining connected with the patient for the total duration of the session.
- For patients in the intervention group, check their scalp condition prior to stimulation via webcam. If the skin is intact, perform the session. For that, have the patients place the SNAPstrap as shown on the training visit.
- Always position the anode SNAPpad situated on the motor cortex (C3 or C4) contralateral to the amputated limb. Ensure that the cathode SNAPpad is located on the supraorbital space, ipsilateral to the amputation side. Encourage the patients to always use a mirror to facilitate collocation and then, turn on the RS-tDCS device.
- Once they are on the stimulation menu, observe that the screen will show the connection quality rated as poor, moderate, or good. When a connection is poor, the device will beep, indicating that no current can be delivered. In that case, have the patients either rearrange the SNAPpads, check for cable connectivity to the device, or add saline solution. Have the patients press the sponges against their skin for 20 s, thus enhancing contact to solve most cases of poor connectivity and start the stimulation when good connectivity appears.
- Provide a code for single-time use to the patients to avoid non-supervised stimulations. During the training session, follow the study protocol with 2 mA intensity for 20 min with a ramp of 30 s to create the stimulation codes on the patient's device. Ensure that these codes remain blinded to the participant to ensure stimulation is delivered within the study context only.
- Always position the anode SNAPpad situated on the motor cortex (C3 or C4) contralateral to the amputated limb. Ensure that the cathode SNAPpad is located on the supraorbital space, ipsilateral to the amputation side. Encourage the patients to always use a mirror to facilitate collocation and then, turn on the RS-tDCS device.
- Once stimulation has been started, complete a 5 min guided meditation consisting of a body scan technique. Begin somatosensory training by following simple and slow movements of the limbs, including movement of the phantom limb until stimulation is complete.
NOTE: Due to safety reasons, to ensure study protocol adherence, this research protocol warrants constant supervision. When possible, the same researcher will be assigned throughout the study for the same participant. - At the end of each session, administer a questionnaire asking about possible side effects and pain levels on a VAS score to the patient (Supplementary File 1). If a patient's pain level is increased by at least 2 points in the VAS scale, (pre-stimulation vs post-stimulation) in two consecutive visits, stop the intervention completely.
- If at any moment of the stimulation, the patient is experiencing severe discomfort or wants to stop the stimulation, ask the subject to abort the session (previously explained during the training session).
Our home-based and remotely supervised protocol is currently being tested in a large, pragmatic, randomized, clinical trial of patients with PLP. Based on previous clinical trial testing in-clinic tDCS in PLP patients, we expect a reduction in the level of PLP, PLS, and RLP compared to the usual care group. This reduction is expected to reach an effect size of at least 0.5, namely a clinically important difference.
Regarding safety outcomes, our initial exploration has shown a similar safety profile to in-site tDCS applications. The most common side effects reported are tingling, itching, and skin redness. Therefore, we expect higher rates of adherence and acceptability in the ongoing study. Moreover, in this protocol, we highlight the feasibility of combining a behavioral intervention with RS-tDCS (e.g., somatosensory training), also combining a home-based biomarker recording such as HRV. We expected that RS-tDCS would significantly modify the HRV compared to the usual care group and hypothesized that the analgesic effect of RS-tDCS in PLP patients would be correlated to an increase in the high-frequency band of the HRV. This modification can be interpreted as an increase in the vagal tonus related to the activation of the endogenous pain modulation system10.
We tested this protocol in two patients with PLP. In this pilot study, twenty sessions were performed, and PLP levels and HRV metrics were measured at home before and after the protocol. Our study showed a significant reduction in PLP intensity levels (p = 0.001, Table 2). This pain reduction is larger than the minimally clinically important difference for chronic pain conditions (reductions of 2 points in a VAS), supporting the analgesic power of this protocol. Similarly, HRV-related variables were modified. As expected, high-frequency HRV significantly increased after the remote protocol (p = 0.003, Table 2) but low-frequency HRV was not. These results suggest an increase in the parasympathetic tonus of patients with PLP.
| Outcome | Pre-treatment | Post-treatment | Difference | p-value |
| PLP VAS | 6.25 ± 0.35 | 2.70 ± 0.42 | -3.55 ± 0.77 | 0.001 |
| HF-HRV | 6.19 ± 0.73 | 9.57 ± 0.60 | 3.38 ± 0.13 | 0.003 |
| LF-HRV | 8.05 ± 0.35 | 6.9 ± 0.14 | -1.15 ± 0.21 | 0.13 |
Table 2: Changes in PLP intensity and heart rate variability (n = 2). Abbreviations: HRV = heart rate variability; PLP = phantom limb pain; HF = High Frequency; LF = Low Frequency; VAS = Visual analog scale.
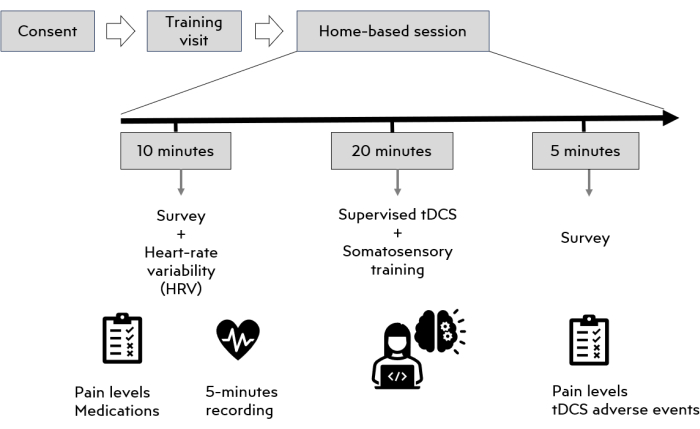
Figure 2: RS-tDCS session structure. Abbreviations: tDCS = transcranial direct current stimulation; RS-tDCS = remotely supervised tDCS. Please click here to view a larger version of this figure.
Supplementary File 1: tDCS side effects questionnaire. Abbreviation: tDCS = transcranial direct current stimulation. Please click here to download this File.
