Once isolated, primary human myofibroblasts can be grown in cell culture and used over a limited number of passages (up to passage 4). These cells are characterized as being a-smooth muscle actin and vimentin positive, and desmin-negative (Figure 1A), consistent with intestinal subepithelial myofibroblasts5,7. They also have a characteristic stellate morphology (Figure 1B). Primary myofibroblasts can then be used to confirm experimental findings identified in a cell line. This approach was utilized to demonstrate that the pro-inflammatory cytokine TNF-α (10 ng/ml) induced the upregulation of EGF receptor expression and signaling in these cells7. Upregulated EGF receptor expression and signaling was initially found utilizing the previously mentioned human colonic myofibroblast cell line 18Co (Figure 2). In Figure 2A, we demonstrate that exposure of 18Co cells to TNF-α led to a time-dependent increase in EGF receptor expression. This correlated with enhanced EGF-induced COX-2 expression and p42/44 MAPK phosphorylation in these cells (Figure 2B). To validate these experimental findings, experiments were repeated using primary human myofibroblasts isolated from surgically resected colon of patients with colorectal cancer. As shown in Figure 2C and 2D, primary human myofibroblasts closely mimic the experimental findings initially identified in the 18Co cell line7.
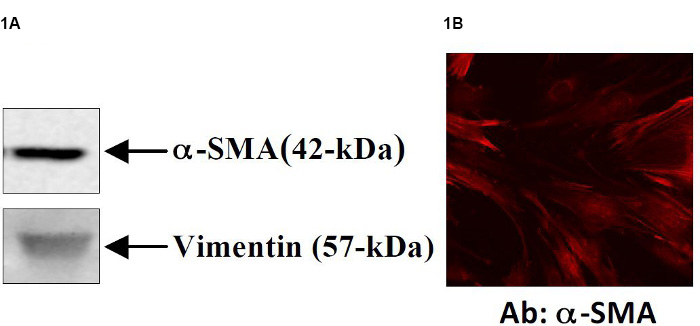
Figure 1. Primary myofibroblasts can be isolated from human colon tissue7. Isolated primary cells demonstrate a myofibroblast-like phenotype that are consistently a-SMA and vimentin positive (Figure 1A) and demonstrate a stellate morphology (Figure 1B).
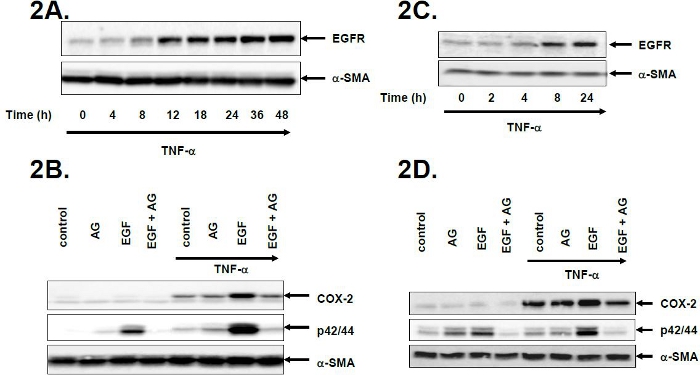
Figure 2. Experimental findings in a cell line are substantiated using primary human myofibroblast cells7. The human colonic myofibroblast cell line 18Co was used to demonstrate that TNF-α induces the upregulation of EGF receptor expression and signaling in these cells (Figure 2A). This upregulation of EGF receptor expression was associated with enhanced EGF receptor signaling, shown in Figure 2B, where subsequent exposure to EGF led to enhanced p42/44 MAPK phosphorylation and COX-2 expression. These effects were completely inhibited with the EGF receptor inhibitor AG1478. Primary human myofibroblasts isolated from surgically resected colon of patients with colorectal cancer confirm these experimental findings (Figures 2C and 2D). Tumor necrosis factor-alpha=TNF-α, EGFR=EGF receptor, AG=AG1478, COX-2=cyclo-oxygenase-2. Click here to view larger figure.
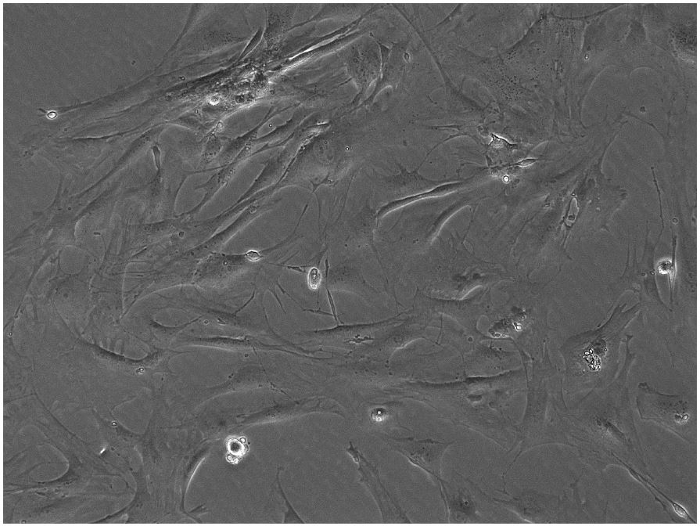
Figure 3. Primary myofibroblasts can be isolated from mouse colon tissue. A 10X view of primary mouse myofibroblast cells. Click here to view larger figure.
