A total of 228 tissue blocks were tested by quantitative polymerase chain reaction (qPCR), which was comprised of 91 cytomegalovirus (CMV) positive cases based on histology and positive immunohistochemistry (IHC), 18 with equivocal CMV IHC, and 79 negative controls. As illustrated in Figure 2, CMV positive cases would have demonstrated typical CMV viral inclusions (A) and/or positive IHC staining (B). Equivocal cases would have demonstrated rare, non-classic appearing staining patterns (C), whereas negative controls would have shown no suspicious histology or IHC staining5.
Of 91 biopsies positive for CMV by histopathology, 88 were positive by qPCR (Table 2). With a true positive definition based on traditional histology, i.e. typical CMV viral inclusions and/or typical CMV IHC, these data resulted in a sensitivity of 96.7%.
Of 79 negative control biopsies (35 normal colon, 25 colitis, and 19 duodenitis), i.e. negative for viral inclusions and negative by CMV IHC, 78 tested negative and 1 tested positive by qPCR, resulting in a specificity of 98.7%.
Fourteen of 18 (78%) biopsies with equivocal CMV IHC staining tested positive for CMV by qPCR5. Among these 18 equivocal cases, eleven had additional biopsies taken the same day that were positive for CMV by histopathology. Among these 14 qPCR positive samples, 10 had biopsies taken the same day that were positive for CMV on histopathology. Of the 18 equivocal biopsies tested, 11 had additional clinical information regarding CMV testing on other specimens submitted at or within 7 days of the time the biopsy was taken. Among these 11 cases, 8 (73%) tested positive for CMV by qPCR. Of these 11 biopsies, 5 (45%) tested positive by qPCR with additional positive CMV specimens; 3 (27%) tested positive by qPCR with no positive CMV specimens; 3 (27%) tested negative by qPCR with additional negative CMV specimens.
In addition to those studies mentioned above, it was of interest to determine whether obtaining additional hematoxylin and eosin (H&E) levels would be beneficial in cases where no viral inclusions are seen on H&E initially and CMV IHC is equivocal. Therefore, H&E levels times 5 for each of the 18 blocks with equivocal CMV IHC were performed. Two pathologists carefully examined these cases and could not identify discernible viral inclusions on any of the additional slides (data not shown).
| Suggested real-time polymerase chain reaction parameters | ||||||
| Setup Readings: | ||||||
| Default Channel | Seek Temperature | Max Seek Pos | Instrument type | Capillary Size | ||
| 530 | 30 °C | 12 | 6 channel | 20 μl | ||
| Program name: Activation of enzyme | ||||||
| Number of cycles: 1 | ||||||
| Analysis mode: None | ||||||
| Target °C | Hold hh:mm:ss | Ramp Rate | Sec Target | Step Size | Step Delay | Acquisition Mode |
| 95 | 0:10:00 | 20 | 0 | 0 | 0 | None |
| Program name: Touch down step | ||||||
| Number of cycles: 10 | ||||||
| Analysis mode: None | ||||||
| Target °C | Hold hh:mm:ss | Ramp Rate | Sec Target | Step Size | Step Delay | Acquisition Mode |
| 95 | 0:00:05 | 20 | 0 | 0 | 0 | None |
| 65 | 0:00:20 | 20 | 55 | 1 | 1 | None |
| 72 | 0:00:15 | 20 | 0 | 0 | 0 | None |
| Program name: Amplification of the DNA | ||||||
| Number of cycles: 40 | ||||||
| Analysis mode: Quantitation | ||||||
| Target °C | Hold hh:mm:ss | Ramp Rate | Sec Target | Step Size | Step Delay | Acquisition Mode |
| 95 | 0:00:05 | 20 | 0 | 0 | 0 | None |
| 55 | 0:00:20 | 20 | 0 | 0 | 0 | Single |
| 72 | 0:00:15 | 10 | 0 | 0 | 0 | None |
| Program name: Cooling | ||||||
| Number of cycles: 1 | ||||||
| Analysis mode: None | ||||||
| Target °C | Hold hh:mm:ss | Ramp Rate | Sec Target | Step Size | Step Delay | Acquisition Mode |
| 40 | 0:00:30 | 20 | 0 | 0 | 0 | None |
Table 1. The parameters listed should be used as a guideline for target temperatures, cycle numbers, and cycle lengths in the set-up of real-time polymerase chain reaction for detecting cytomegalovirus in formalin-fixed, paraffin-embedded gastrointestinal biopsies. These parameters may require optimization depending on the instrument model and manufacturer.
| Histology Positive Cases | PCR Positive Cases | Sensitivity | Histology Negative Cases | PCR Negative Cases | Specitivity |
| 91 | 88 | 96.7% | 79 | 78 | 98.7% |
Table 2. Sensitivity (96.7%) and specificity (98.7%) of real-time polymerase chain reaction (qPCR) at detecting cytomegalovirus in formalin-fixed, paraffin-embedded gastrointestinal biopsies. This table has been modified from McCoy et al5.
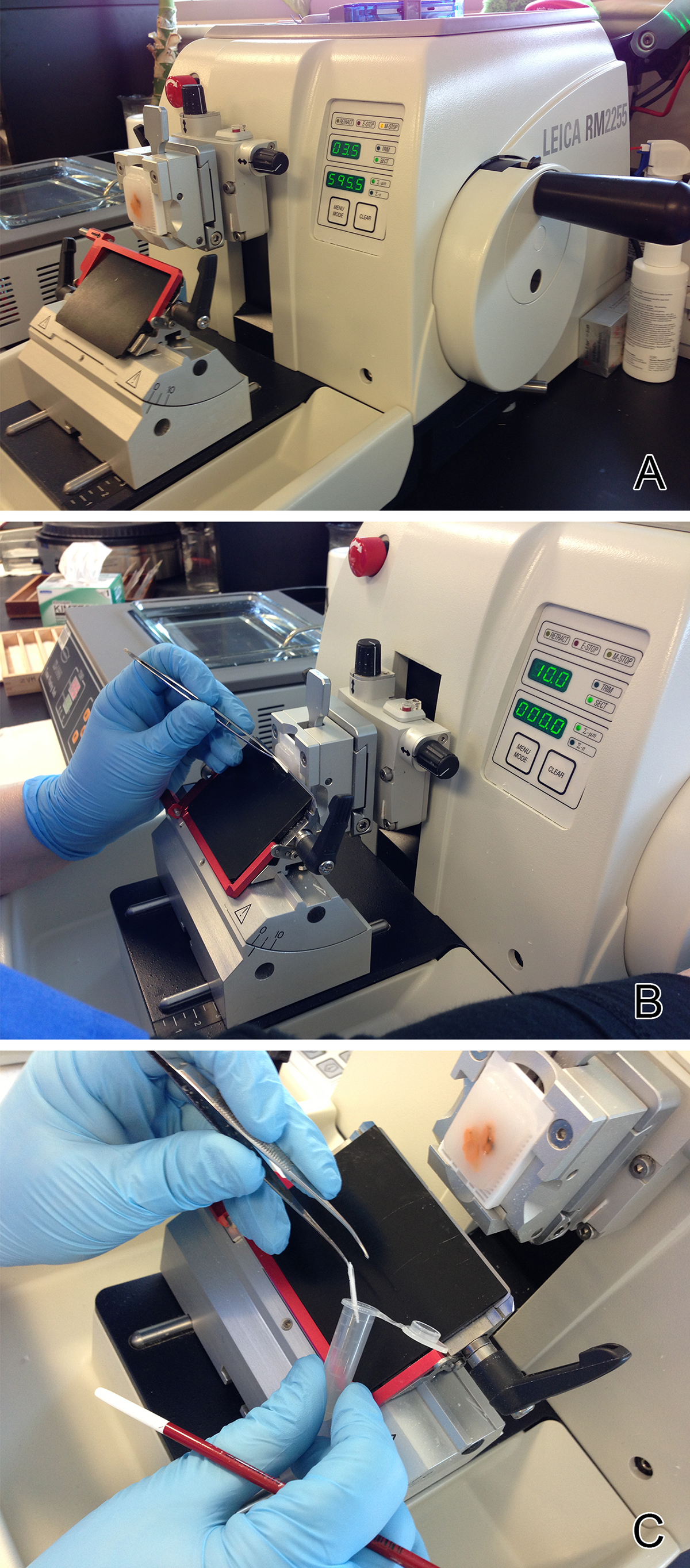
Figure 1. A typical microtome with the tissue block seated correctly in the cassette clamp A) As a 10 micron thick section of biopsy tissue is cut it is allowed to roll into a scroll B), which is transferred to a microfuge tube C). All five scrolls of biopsy tissue are placed in a single microfuge tube for DNA extraction.
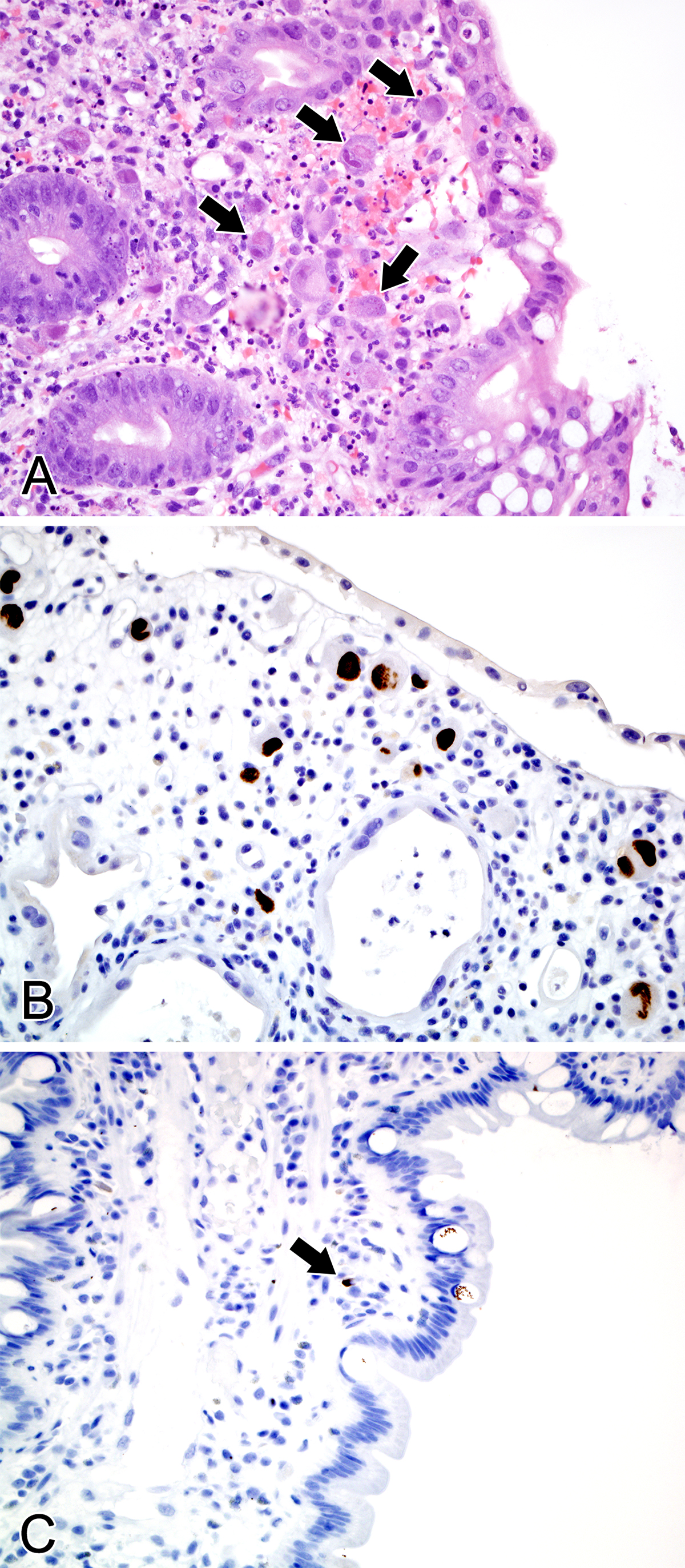
Figure 2. A) Hematoxylin and eosin stained section of a colon biopsy showing abundant, typical CMV inclusions as indicated by arrows (original magnification 400X). B) A colon biopsy stained with a monoclonal antibody against CMV showing the expected IHC staining pattern (original magnification 400X). C) A colon biopsy showing equivocal IHC staining, with a single, small weakly stained cell indicated by the arrow (original magnification 400X). This figure is being reprinted with permission from McCoy et al5.
