In Vitro Modeling of Cancerous Neural Invasion: The Dorsal Root Ganglion Model
Summary
This video article shows the use of the dorsal root ganglia (DRG)/cancer cell model in pancreatic ductal adenocarcinoma.
Abstract
One way that solid tumors disseminate is through neural invasion. This route is well-known in cancers of the head and neck, prostate, and pancreas. These neurotropic cancer cells have a unique ability to migrate unidirectionally along nerves towards the central nervous system (CNS). The dorsal root ganglia (DRG)/cancer cell model is a three dimensional (3D) in vitro model frequently used for studying the interaction between neural stroma and cancer cells. In this model, mouse or human cancer cell lines are grown in ECM adjacent to preparations of freshly dissociated cultured DRG. In this article, the DRG isolation protocol from mice, and implantation in petri dishes for co-culturing with pancreatic cancer cells are demonstrated. Five days after implantation, the cancer cells made contact with the DRG neurites. Later, these cells formed bridgeheads to facilitate more extensive polarized, neurotropic migration of cancer cells.
Introduction
Solid tumors disseminate in three main ways: direct invasion, lymphatic spread, and hematogenic spread. However, there is a fourth means of cancer spread that is frequently disregarded, dissemination along nerves. Cancerous neural invasion (CNI) is a well-known route of cancer spread, especially in cancers of the head and neck,1 prostate2, 3 and pancreas.4-8 CNI occurs in more than 80% of individuals with pancreatic adenocarcinoma, leading to retroperitoneal tumor spread through celiac ganglion nerves. These neurotropic cancer cells have a unique ability to migrate unidirectionally along nerves towards the central nervous system (CNS).9 This finding suggests that the perineural microenvironment can be exploited by cancer cells, providing factors that support malignant growth.
One of the few in vitro models for CNI research is the dorsal root ganglia (DRG)/cancer cell model. This model is frequently used for studying the paracrine interaction between neural stroma and cancer cells.10-18 In this model, mouse or human cancer cell lines are grown in extracellular matrix (ECM) adjacent to preparations of freshly dissociated cultured DRG.
This video article shows the application of in vitro CNI in pancreatic ductal adenocarcinoma.
Protocol
Four- to six-week-old female C57BL/CJ mice (Harlan, Jerusalem, Israel) were used in the experiment according to the Association for Assessment and Accreditation of Laboratory Animal Care specifications. All experimental procedures were done in accordance with Institutional Animal Care and Use Committee and the Department of Agriculture regulations.
1. Harvesting the Spinal Cord
- Euthanize the mouse using a CO2 chamber. Avoid cervical dislocation as it might cause damage to the ganglion roots due to shear forces. From here on, perform all steps under sterile conditions.
- Soak animal down with 70% ethanol. This step is important for sterilization and for preventing the hair from dragging through the inner organs.
- Leave the mouse to dry from ethanol. Prevent any contact of ethanol with the inner organs due to neurotoxicity.
- After drying the mouse, position it using pins in prone position (face down). Place the pins on each hindlimb and forelimb.
- Using forceps, make a midline incision extending craniocaudally from the posterior neck to the lumbar spine. Next, raise dermal flaps bilaterally using forceps and expose subcutaneous tissue.
- Palpate mouse skull until reaching the craniocervical junction. Using scissors perpendicular to the animal, cut through the cervical muscles and spine at the craniocervical junction (the 7th cervical vertebrae), using heavy forceps. Dissect the spine caudally and excise the spine with heavy forceps until reaching the lumbar level (hind limbs level).
- Perform a complete caudal transection at the lumbar spine level (the 5th lumbar vertebrae) using heavy forceps.
- Roll the mouse over (face up). There is no need to cover the incision since the DRG is extracted from lower vertebral levels and not the cervical.
- Cut down at the midline from the neck to the abdomen, retract the skin laterally and then cut to open the peritoneum.
- Remove the inner organs inside the peritoneum (liver, spleen, pancreas, stomach, and intestine) en bloc. Next, remove the retroperitoneal organs (i.e., kidneys and pancreas). Cranially, open the chest wall.
- Using forceps and a surgical blade, cut the ribs, leaving 5 mm of ribs bilaterally away from the vertebral column. At this point, the vertebral column is separated from the rest of the body.
- Wash the vertebral column from blood with cold (4 °C) fresh phosphate buffered saline (PBS) twice.
2. Isolating the Dorsal Root Ganglia (DRG)
- Use a stereomicroscope with 4X magnification.
- Position the spine on a non-adherent non absorbing platform (Telfa/nylon). Position the spine face up at the same cranio-caudal orientation.
- Remove any spinal muscles and connective tissue. Use the ribs as a landmark for nerves as they leave the spine. Ribs also protect the nerves from the surgical tools. The DRG are located at the cervical, thoracic, and lumbar sites of the vertebrae.
- Next, using scissors cut the vertebral body in the midline and expose the spinal cord and DRG roots by gentle lateral retraction of the vertebral body.
- In the intercostal space, follow the peripheral nerve medially along the rib lateral to the DRG.
- Identify the DRG. It looks like the yolk of 'fried egg' lying on the nerve.
- Cut the intercostal nerve distal to the DRG leaving 2-3 mm of nerve distal to the ganglia, to be used for retraction. This "tail" will be removed after harvesting.
- Grasp the nerve using forceps. Pinching the DRG body itself will cause neural cell damage and should be avoided.
- Approach the DRG proximally along its attachment to the spinal cord, via its anterior and posterior roots.
- Apply gentle retraction to the DRG by pulling the efferent nerve (intercostal nerve stump) laterally, and cut the anterior and posterior roots close to the DRG.
- Keep the DRG in a 35 mm Petri dish filled with fresh, ice cold DMEM supplemented with 10% fetal calf serum (FCS), 1% penicillin-streptomycin, 1% non-essential amino acids, and 1% Sodium pyruvate.
3. Implantation in the Petri Dish
- Perform the next steps on ice using pre-cooled pipette tips to prevent ECM solidification.
- Under a stereomicroscope at 2-4X magnification, place a 35 mm glass bottom petri dish on a paper grid.
IMPORTANT: Work on ice in order to keep the ECM in liquid state. Create a 1 mm diameter spot (approximately 20 µl) of growth factor-depleted ECM at the center of the grid. - Under direct visualization, place the DRG at the center of the ECM spot close to the bottom of the dish.
Note: The cancer cells used in this protocol are murine pancreatic cancer cells (KPC) established from freshly isolated tumor specimens from KPC mice as described elsewhere19. - Harvest 40,000 cancer cells from confluent cultures, wash them once with PBS, and resuspend them in 40 µl ECM on ice.
- Under direct visualization of the grid using a stereomicroscope measure 500 µm at each direction from the DRG. At this point slowly seed 10,000 cells/10 µl ECM. Use a 2-10 µl precooled tip to inject the cells close to the dish bottom, avoiding their spread in the matrix or detachment of the matrix. (Figure 1).
- Leave the dish within a laminar flow hood for 10-15 min to solidify. Avoid ECM drying.
- Slowly add DMEM, prepared as previously mentioned, against the side wall of the plate. Add enough medium to cover the ECM (about 2 ml).
- Put the dish back to the incubator at 37 °C.
- Replace the medium with fresh medium on the following day.
- Replace the medium every 2 days.
4. Data Acquisition, Time-lapse Videomicroscopy
- On day 7 after the implantation, take the dish for time lapse microscopy. Note that certain cells might require acquisition earlier due to faster migration.
- During the live imaging, place the dish in a closed environment at a mean temperature of 37 ±0.1 °C and 5% CO2.
- Record the cells by using a charge coupled device camera placed on the microscope.
- Take digitized images every 10 min for up to 72 hr to follow cell locomotion from three to six different cells.
- Replace medium after 24 hr.
- Perform data acquisition and simple analysis using the microscope software.
5. Data Analysis
- For more advanced applications (i.e., cell tracking in 2D or 3D) use specialized software (such as Imaris 4D). Note: This software determines the xy coordinates of a cell at any given time, along with the distance from origin, and speed of motion.
- Calculate the mean velocity by measuring the travel distance between subsequent positions in 10 min intervals. Calculate the Forward Migration Index (FMI) which is the distance of the cell front from the neurite and describes the unidirectional movement of the cells toward the DRG.
Representative Results
Using video microscopy imaging, the DRG can be seen sprouting neurites 5-7 days after implantation while the cancer cells migrating away from their colonies toward the DRG. By the 7th day after the implantation, the cancer cells come in contact with the neurites (Figure 2).
The Forward migration index of the pancreatic cancer cells used in the protocol is 3-4 fold higher than that of other cell lines (QLL2, B16F) (Figure 3a). Figure 3b presents a representative X and Y coordinate graph, depicting the migration path of a KPC cancer cell in contact with the nerve; time-lapse videomicroscopy analysis showed differences in the forward movement but not velocity between the KPC cells and non-invading cells (Figure 3c-d).

Figure 1: Schematic Illustration of the Protocol Steps. Please click here to view a larger version of this figure.
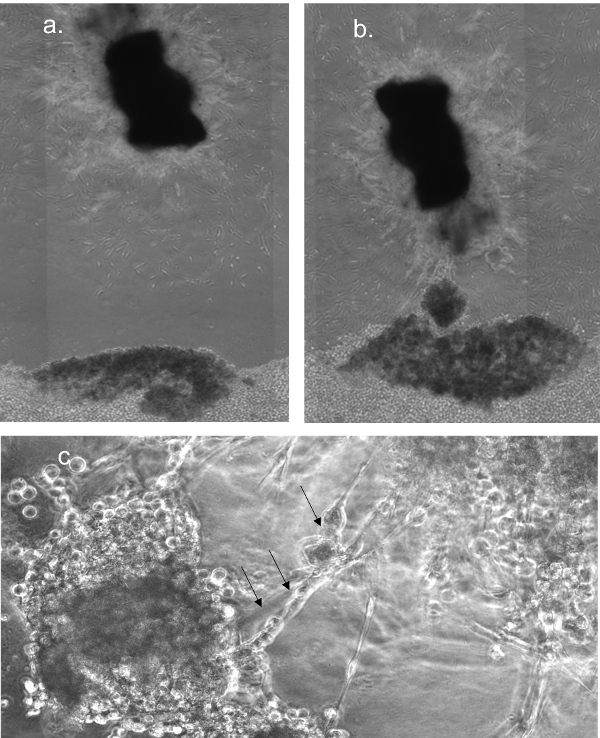
Figure 2: Cancer Cell Invasion Along the Neurons of the DRG. (a) DRG (top) and cancer cells (bottom) on day 0 after seeding (5X magnification). (b) DRG and cancer cells on day 7 after seeding (5X magnification). (c) Cancer cells migrate along the DRG neuron (arrows). All bars represent 50 µm. Please click here to view a larger version of this figure.
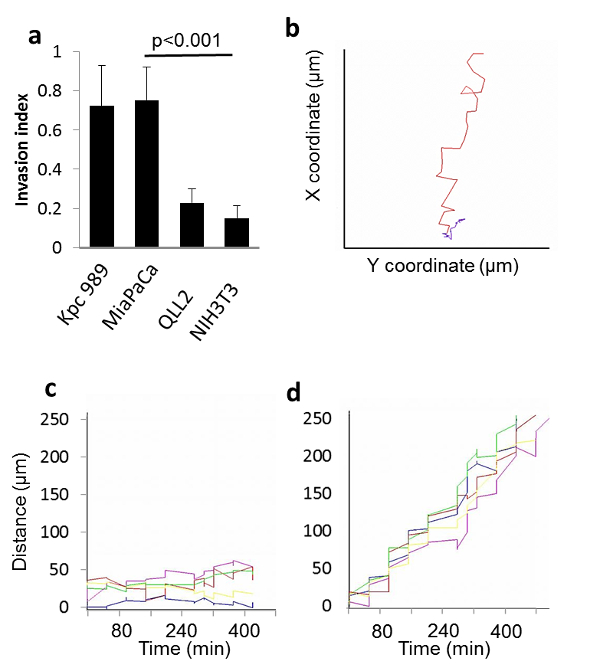
Figure 3: Dorsal Root Ganglion (DRG) Neurons Induce CNI. (a) Nerve invasion index of MiaPaCa2 cancer cells , KPC cells, QLL2, and NIH3T3 cells. (b) A coordinate graph depicting the migration path of a KPC cancer cell in contact with the nerve (red) and QLL2 cell (purple). The Y and X coordinates are shown. (n = 12-20 in each group). (c) Analysis of distance from origin of migrating QLL2 cancer cells with axonal contact and (d) KPC cancer cells (n = 20). The direction of migration was constantly toward the nerve ganglion. P values in (a) were calculated by two-sided Student t test. Please click here to view a larger version of this figure.
Discussion
This article presents an in vitro model that recapitulates the cancerous microenvironment in the neural niche, the DRG model. The video demonstrates all the steps starting from recognizing anatomical landmarks such as the DRG in the mouse, its extraction, and finally, its culturing in ECM. Co-culturing the DRG alongside with cancer cells is also presented. There are no other models for in vitro perineural invasion research described in the literature making this model essential for studying the perineural niche microenvironment in vitro.
The protocol presented in the video has two critical steps. First, care should be taken when grasping the nerve adjacent to the DRG body (step 2.7 in the protocol). Grasping or pinching the DRG might cause irreversible mechanical or ischemic damage to the DRG preventing it from growing and sprouting when seeded in the Petri dish. The second critical step is the implantation of the cancer cells in the Petri dish inside the ECM. It is important to seed the cells slowly and with caution, to avoid the floating of cells and their spread over the Petri dish. The aim of the implantation is to localize the cells in one place, to facilitate tracking their movement (distance and direction).
Once established the model microenvironment can be modified according to the tested hypothesis. For instance, adding a third cell culture to the Petri dish (for example, non-cancerous cells) enables the researcher to compare the neurotropic migration capabilities of different cells. Furthermore, the researcher can apply different conditions (i.e., temperature, humidity, soluble factors, etc.) and examine their effect on the cells invasion ability.
The DRG model enables the researcher to study the interaction between cancer cells and nerves. It is also used for time lapse experiments in which morphological changes in the perineural niche are demonstrated in a temporal fashion. Furthermore, the neuroinvasive cells can be subjected to various treatments and their effect on the interaction with neurites of the ganglia can be assessed.
Not every cell line is suitable for the DRG model. They should be cancer cells with the intrinsic ability to invade through nerve and to degrade ECM. Furthermore, note that each cancer cell type has different invasion characteristics and so the time the cells are expected to make contact with the DRG neurites varies. For example, The KPC cells we used need about 7 days to invade through the ECM toward the DRG whereas MiaPaca cells (human pancreatic adenocarcinoma cells) need only 72-96 hr to make that contact.
A limitation of this model includes the possible incompatibility with human cells. Due to its use of mouse DRG, the mouse-human protein-protein interaction cannot always be demonstrated when human cancer cells are used. Whenever planning to use this model with the two different species, the homology of the examined protein should be tested and if there is high homology the assay is supposed to be suitable for evaluating protein-protein interactions. As well, it should kept in mind that the DRG assay as proposed in this protocol represents the neural microenvironment including other cells, not only neurons (i.e., Schwann cells, fibroblasts, macrophages, etc.). Hence, specific cell populations cannot be tested specifically.
Disclosures
The authors have nothing to disclose.
Acknowledgements
Edith Suss-Toby is thanked for her assistance in the time-lapse microscopy and image analysis. Nofar Rada is thanked for the artistic work.
Materials
| Equipments: | |||
| Operating microscope | Leica | M205 | |
| Tiime Lapse System | Zeiss | ||
| Forceps | Sigma-Aldrich | F4142 | |
| Surgical blade | Sigma-Aldrich | Z309036 | |
| Scissors | Sigma-Aldrich | S3271 | |
| 35mm petri dishes, glass bottom | de groot | 60-627860 | |
| Name | Company | Catalog Number | Comments |
| Materials: | |||
| 70% ethanol | sigma | ||
| Cold PBS | Biological industries | 02-023-1A | |
| DMEM | Biological industries | 01-055-1A | |
| FCS | Rhenium | 10108165 | |
| Penicillin and streptomycin | Biological industries | 01-031-1B | |
| Sodium Pyruvate | Biological industries | 03-042-1B | |
| L-Glutamine | Biological industries | 03-020-1B | |
| Growth factor depleted matrigel | Trevigen | 3433-005-01 |
References
- Carter, R. L., Foster, C. S., Dinsdale, E. A., Pittam, M. R. Perineural spread by squamous carcinomas of the head and neck, a morphological study using antiaxonal and antimyelin monoclonal antibodies. J Clin Pathol. 36, 269-275 (1983).
- Beard, C. J., et al. Perineural invasion is associated with increased relapse after external beam radiotherapy for men with low-risk prostate cancer and may be a marker for occult, high-grade cancer. Int J Radiat Oncol Biol Phys. 58, 19-24 (2004).
- Maru, N., Ohori, M., Kattan, M. W., Scardino, P. T., Wheeler, T. M. Prognostic significance of the diameter of perineural invasion in radical prostatectomy specimens. Hum Pathol. 32, 828-833 (2001).
- Ceyhan, G. O., et al. Pancreatic neuropathy and neuropathic pain–a comprehensive pathomorphological study of 546 cases. Gastroenterology. 136, 177-186 (2009).
- Ceyhan, G. O., et al. The neurotrophic factor artemin promotes pancreatic cancer invasion. Ann Surg. 244, 274-281 (2006).
- Takahashi, T., et al. Perineural invasion by ductal adenocarcinoma of the pancreas. J Surg Oncol. 65, 164-170 (1997).
- Zhu, Z., et al. Nerve growth factor expression correlates with perineural invasion and pain in human pancreatic cancer. J Clin Oncol. 17, 2419-2428 (1999).
- Hirai, I., et al. Perineural invasion in pancreatic cancer. Pancreas. 24, 15-25 (2005).
- Mitchem, J. B., et al. Targeting tumor-infiltrating macrophages decreases tumor-initiating cells, relieves immunosuppression, and improves chemotherapeutic responses. Cancer Res. 73, 1128-1141 (2013).
- Kelly, K., et al. Attenuated multimutated herpes simplex virus-1 effectively treats prostate carcinomas with neural invasion while preserving nerve function. FASEB J. 22, 1839-1848 (2008).
- Dai, H., et al. Enhanced survival in perineural invasion of pancreatic cancer, an in vitro approach. Hum Pathol. 38, 299-307 (2007).
- Ayala, G. E., et al. Cancer-related axonogenesis and neurogenesis in prostate cancer. Clin Cancer Res. 14, 7593-7603 (2008).
- Ayala, G. E., et al. Stromal antiapoptotic paracrine loop in perineural invasion of prostatic carcinoma. Cancer Res. 66, 5159-5164 (2006).
- Ceyhan, G. O., et al. Neural invasion in pancreatic cancer, a mutual tropism between neurons and cancer cells. Biochem Biophys Res Commun. 374, 442-447 (2008).
- Bapat, A. A., Hostetter, G., Von Hoff, D. D., Han, H. Perineural invasion and associated pain in pancreatic cancer. Nat Rev Cancer. 11, 695-707 (2011).
- Ketterer, K., et al. Reverse transcription-PCR analysis of laser-captured cells points to potential paracrine and autocrine actions of neurotrophins in pancreatic cancer. Clin Cancer Res. 9, 5127-5136 (2003).
- Gil, Z., et al. Nerve-sparing therapy with oncolytic herpes virus for cancers with neural invasion. Clin Cancer Res. 13, 6479-6485 (2007).
- Gil, Z., et al. Paracrine regulation of pancreatic cancer cell invasion by peripheral nerves. J Natl Cancer Inst. 102, 107-118 (2010).
- Weizman, N., et al. Macrophages mediate gemcitabine resistance of pancreatic adenocarcinoma by upregulating cytidinedeaminase. Oncogene. 33, 3812-3819 (2014).
