We optimized the experimental protocol of IR surgery to obtain reproducible IR induced injury of the ileum in mice. Representative results are demonstrated in this section.
Figure 1 shows examples of microvascular clips position to induce ischemia of the ileum. Black arrows show position of the main clips occluding first order branches of superior mesenteric artery. Green arrows show the position of additional clips to block blood supply from collateral vessels. Note increased size of occluded vessels distal to the clips position and color change of the ischemic region of intestinte. After removal of the clips at the end of ischemia blood vessels regain blood flow and return to normal size.
Figure 2 shows an example of a tissue cassette containing Swiss rolls prepared from control and ischemic regions of the ileum after 1 hr of ischemia, followed by a 1 hr of reperfusion. A piece of spleen was included to facilitate positioning of control and IR intestine during processing and staining. Note the color difference between control and ischemic tissue.
Figure 3 shows representative hematoxylin and eosin staining of control and ischemic regions of the ileum after 1 hr of ischemia, or 1 hr of ischemia followed by a 2 hr of reperfusion. Note the severe damage of the epithelium after 1 hr of ischemia characterized by hemorrhagic villi, epithelium denudement with partial to complete ablation of crypts, and immune cell infiltration (asterisk). After a 2 hr of reperfusion villi damage and inflammation persist (asterisk), but there is no tissue hemorrhage.
Figure 4 shows an example of the analysis of inflammatory cytokines expression at 1 hr and 2 hr after ischemia-reperfusion in ischemic and control intestine. Note upregulation of mRNA expression of TNF, IL-1b, IL-6 and CXCL2 at 1 hr and 2 hr after ischemia-reperfusion compared to control healthy tissue.
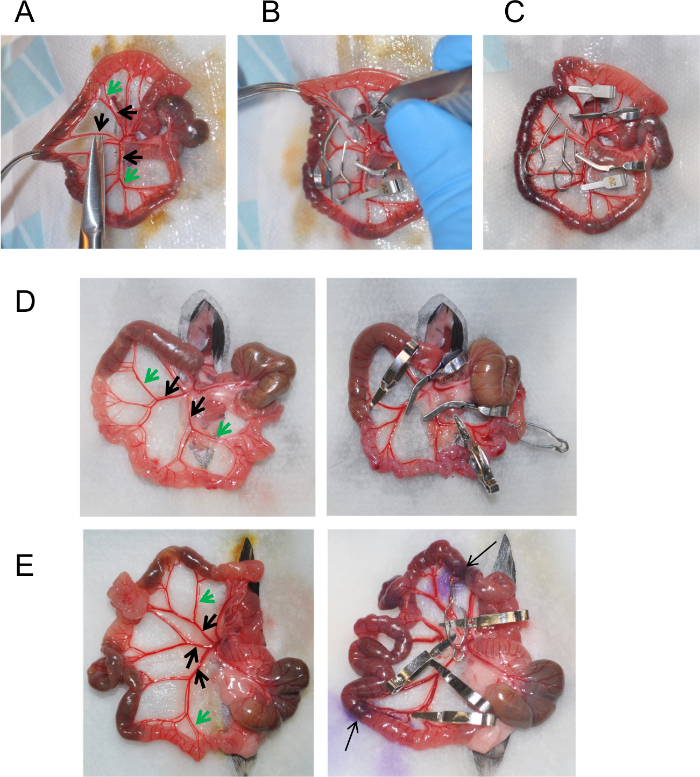
Figure 1: Induction of Ischemia using Vascular Clips. (A) Isolated area of the intestine containing cecum and ileum. Small cuts in the mesentery surrounding the superior mesenteric artery are made to facilitate clip application. (B) Microvascular clip application using clip applier. (C) Position of microvascular clips on superior mesenteric artery to induce ischemia. (D, E). Examples of vasculature structure and clip positioning in different mice. Arrows indicate the ischemic area of ileum marked by hematoxylin. Please click here to view a larger version of this figure.
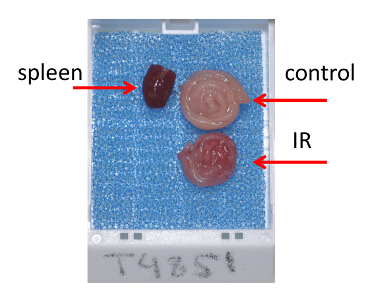
Figure 2: Tissue Preparation for Histological Analysis. Tissue cassette containing Swiss rolls prepared from ischemic and control regions of the ileum after 1 hr of ischemia followed by a 1 hr of reperfusion. Please click here to view a larger version of this figure.
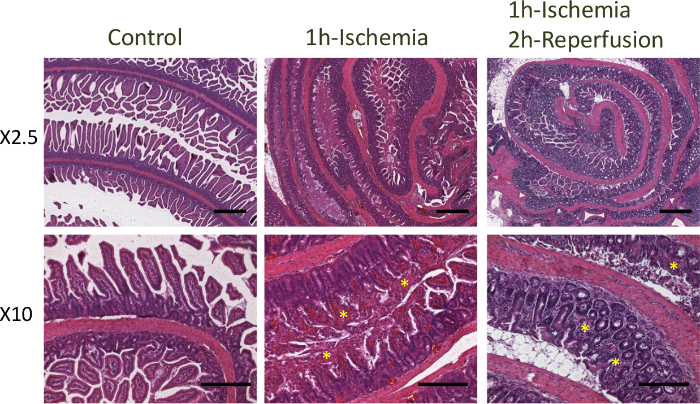
Figure 3: Hematoxylin and Eosin Staining of Ileum after Ischemia. Hematoxylin and eosin staining of control and ischemic regions of the ileum after 1 hr of ischemia, or 1 hr of ischemia followed by a 2 hr of reperfusion. Bars = 500 μm (top panels), 200 μm (bottom panels). Please click here to view a larger version of this figure.
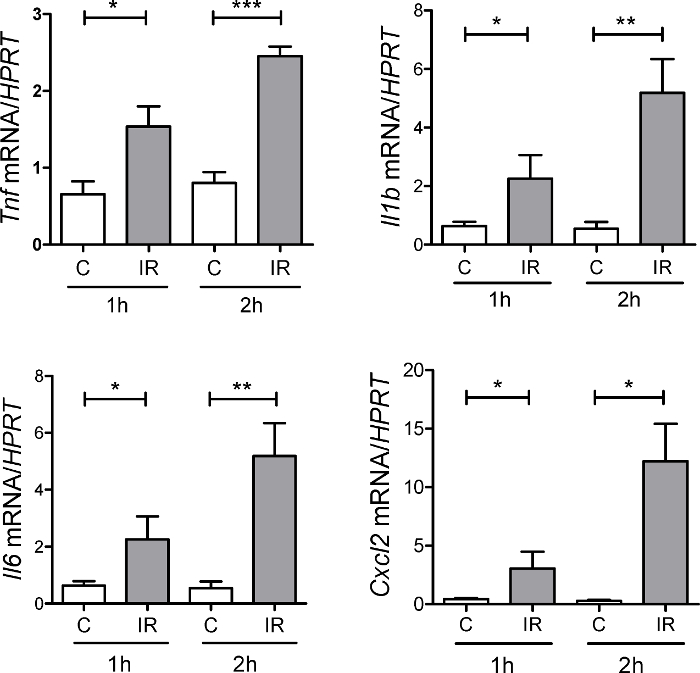
Figure 4: Expression of Inflammatory Cytokines During Ischemia-Reperfusion. Expression of CXCL2, TNF, IL-6, IL-1b was measured at 1 hr and 2 hr after ischemia-reperfusion in ischemic tissue (IR) and normal control tissue (C) adjacent to the ischemic region by real-time PCR. n = 3 – 8 mice per group, * p <0.05; ** p <0.01; *** p <0.001. Error bars represent s.e.m. Please click here to view a larger version of this figure.
| Murine Species | Anesthesia / Analgesia | Artery occlusion method | Ischemia time | Time after reperfusion | Reference | |||
| Sprague-Dawley rats | Sodium pentobarbital | Occlusion of SMA and celiac artery using aneurysm clip or clamp | 45 min | 2 hr | 12 | |||
| C57Bl6/129 | 2% halothane | Occlusion of mesenteric arteriole, and the proximal and distal portions of the ischemic tissue. | 30 to 130 min | 6 hr | 13 | |||
| C57BL/6 | Ketamine, Isoflurane | Occlusion of SMA using aneurysm clips. Occlusion of collateral circulation at the proximal and distal areas. | 1 hr | 1.5 hr | 4,8,11 | |||
| C3H/Hej | Sodium pentobarbital | Occlusion using aneurysm clip or clamp | 40 min | 6 hr | 14 | |||
| C56BL/6 | Isoflurane | Occlusion of SMA and ileocolic artery using aneurysm clip or clamp | 100 min | 1, 2, 4, 24 hr | 15 | |||
| C57BL/6 | Urethane | Occlusion using aneurysm clip or clamp | 45 min | 60 min | 16 | |||
Table 1: Variations in Methodology in Murine Intestinal IR-induced Injury
| Histology scoring system | Reference | ||
| Grade 0: Normal mucosa | 13,17,18 | ||
| Grade 1: Subepithelial space at the villous tip | |||
| Grade 2: More extended subepithelial space | |||
| Grade 3: Epithelial lifting along the villous sides | |||
| Grade 4: Denuded villi | |||
| Grade 5: Loss of villous tissue | |||
| Grade 6: Crypt layer infarction | |||
| Grade 7: Transmucosal infarction | |||
| Grade 8: Transmural infarction | |||
| Grade 0: Normal mucosa | 4,8,11,19-21 | ||
| Grade 1: Sloughing of cells on villous tips | |||
| Grade 2: Mid-villous damage | |||
| Grade 3: Villi were absent, but crypts were still readily detectable | |||
| Grade 4: Complete absence of epithelial structures and transmural necrosis | |||
| Grade 0: Normal villus | 6,22-31 | ||
| Grade 1: Villi with tip distortion | |||
| Grade 2: Goblet cells and Gugenheims' spaces are missing | |||
| Grade 3: Villi with patchy disruption of the epithelial cells | |||
| Grade 4: Villi with exposed, but intact lamina propria with epithelial cell sloughing | |||
| Grade 5: Lamina propria is exuding | |||
| Grade 6: Villi that display hemorrhage or to villi that are denuded | |||
| Grade 0: Normal histology | 32,33 | ||
| Grade 1: Slight disruption of the surface epithelium | |||
| Grade 2: Epithelial cell loss injury at villus tip | |||
| Grade 3: Mucosal vasocongestion, hemorrhage, and focal necrosis with loss of less than half of villi | |||
| Grade 4: Damage extending to more than one-half of villi | |||
Table 2: Histology Scoring Systems in Murine Intestinal IR-induced Injury
