All experiments have complied with the National Institutes of Health Guide for the Care and Use of Laboratory Animals (NIH Publications No. 80023, revised 1978). The procedure was approved with IACUC protocol #2016-0068 by the Cincinnati Children's Research Foundation Institutional Animal Care and Use Committee.
1. Preparation
- To mate age-matched wild-type (WT) C57BL/6 mice, place them in the same cage at 6:00 p.m. and separate them at 9:00 a.m. the next day.
- To determine embryonic day 0 (E0), look at the vaginal plug, which has a homogeneous outer zone attached to the vaginal wall and an inner zone that is fibrous and includes some spermatozoa that form entangled masses mixed with the fibers of the plug material.
- Record the weight of the mice at the time of mating.
- Re-weigh the mice on E10 to ensure ongoing pregnancy.
- Perform the surgery on E16.5 (early canalicular stage).
- Sterilize the instruments that are going to be used during surgery: scissors, needle holder, forceps, clamps, and surgical knives and handles.
- Pre-heat the surgery platform to 24 °C and prepare warm saline (24 °C) prior to surgery.
- Create a warm environment for recovery, and leave wet food inside the cage for the early feeding.
- Stay with the operated animals until they can feed themselves.
- Keep the operated mice alone in their individual cages after the surgery.
2. Anesthesia
- Apply subcutaneous 0.1 mg/kg of buprenorphine to the pregnant dams 1 h before the procedure.
- Use inhaled 5 mL/h of isoflurane for induction and 2 mL/h continuously during the procedure for anesthesia.
- Monitor the movements of the chins of the pregnant mice.
3. Laparotomy
- Clean the abdominal surface with alcohol and povidone-iodine. Maintain sterile conditions throughout the operation.
- Perform a vertical incision for the laparotomy of pregnant dams. Cut all layers separately.
- Identify uterine horns on each side.
- Determine the candidate fetuses for the surgery.
NOTE: Do not operate on the fetuses that are the nearest to the vagina. - Operate on two fetuses in each uterine horn if there are an even number of fetuses on each side (4 most of the time), and on 1 fetus in each uterine horn if there are an odd number of the uterus(3 most of the time).
4. Tracheal occlusion
- Use 2.5x magnification glasses for visualization.
- Position the uterine horn in a transverse fashion.
- Take the pups, facing upward, between two fingers using the eyes of the pups and the tail as a guide to position the fetus.
- Apply gentle pressure to the pup's head to allow extension of the head and therefore, visualization of the neck.
- Use a 6.0 polypropylene suture with an atraumatic needle to perform TO (Figure 1). Keep the placenta on the side and far from the entrance and exit points of the needle.
- Insert the needle transversely through the side of the uterus away from the placenta through the 1/3rd anterior part of the neck.
- Move the needle gently until the midline of the neck and direct it to the anterior part, then exit the neck between the trachea and opposite the carotid sheath and uterus.
- Knot the suture, taking care to maintain the integrity of the membranes and uterine wall, and keep the umbilical cord safe during knotting.
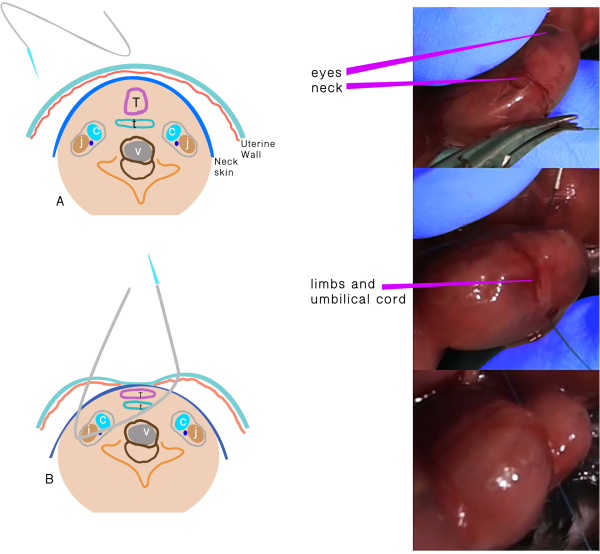
Figure 1: Tracheal occlusion. (A) The transuterine suture passing through the neck. (B) Schematic representation of the structures after the suture passes through and before the knot. Abbreviations: C = Carotid artery; J = Jugular vein; T =Trachea; E = Esophagus; V = Vertebra. Please click here to view a larger version of this figure.
5. Abdominal wall closure
- Replace the uterine horn in the abdomen.
- Inject 2 mL of warm sterile saline into the peritoneal cavity before closure.
- Put a running 5/0 polyglactin suture to close the abdominal wall, and close the skin with a non-running silk suture.
- Apply 0.1 mg/kg of buprenorphine intraperitoneally for analgesia, and allow the recovery of the dam in a warm incubator.
6. Harvest
- Apply anesthesia to the pregnant dam, and harvest all fetuses at E18.5 by cesarean section.
- Check the viability of the fetuses by watching the movements of the fetuses.
- Use at least two different techniques for the euthanasia: carbon dioxide insufflation and cervical dislocation.
- Remove the bodies per the regulation of veterinary laboratory.
- Weigh all fetuses.
- Perform a vertical incision on the thorax for thoracotomy to remove the lungs.
- Dissect the lungs of embryos, and weigh them to calculate total lung to body weight ratio (LBWR = (left lung weight + right lung weight)/body weight x100).
7. Histology
- Snap-freeze the tissues in liquid nitrogen, optimal cutting temperature compound, and dry ice.
- Cut the samples in 10 µm sections using a cryostat, and mount them on poly-lysine-coated slides.
- Bake the slides at 60 °C overnight, and stain the baked slides with hematoxylin and eosin before mounting them for image acquisition at 10-20x magnification using a widefield microscope.
8. Tissue processing for protein and DNA analyses
- Snap-freeze the dissected fetal lungs, and homogenize them in 300 µL of radioimmunoprecipitation assay buffer. Centrifuge at 4 °C for 5 min at 18,000 × g.
- Extract and quantify protein, DNA, and RNA10,12.
This study examined 37 fetuses: 20 (54.1%) as TO vs. 17 (45.9%) as control. As the trachea could not be occluded in 4 fetuses in the TO group, they were excluded from the study. There was no significant difference in mortality in both groups: 4 fetuses (25%) in the TO group and 2 fetuses (12%) in the control group (p=0.334, odds ratio (OR) 2.5, 95% confidence interval (CI) 0.39-16.05). The mean body weight, lung weight, and lung to body weight ratio (LBWR) were higher in the TO group than in the control group (Table 1). There was a significant difference in LBWR (p=0.006) between the TO and control groups.
DNA, RNA, and protein were quantified to determine the reason for the difference in LBWR (Figure 2). Lung DNA amounts and the DNA/protein ratio were higher in the TO group, no difference was observed in lung RNA, and protein amounts were lower in the TO group than in the control group,as previously observed in the rabbit TO model in which epithelial hyperplasia was noted12. The diameters of the airways in the TO group also demonstrated an increase.
Histological analyses of the E18.5 lungs showed the late canalicular/early saccular stage of lung development with developing airspaces and thickened interstitium between epithelial surfaces in the control samples while the lungs in the TO group had dilated central and distal airspaces with subjectively higher numbers of nuclei (Figure 2). This increased cellularity is consistent with the noted increase in the amount of lung DNA.
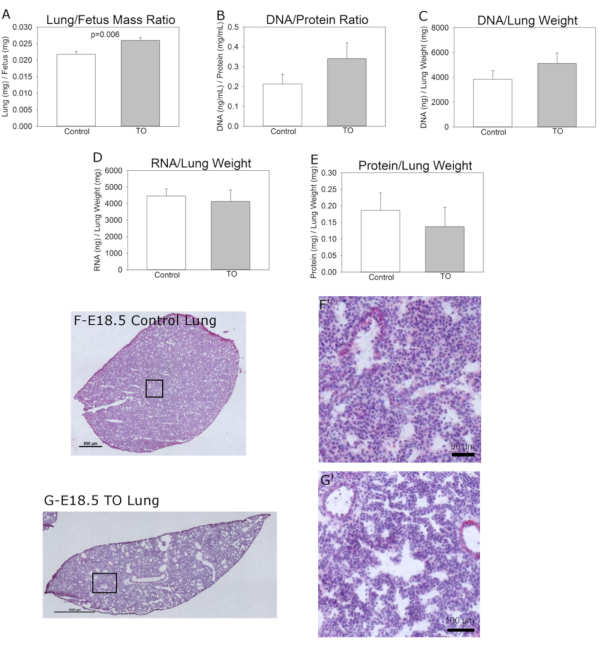
Figure 2: Features of the groups. (A) Normalized lung to fetus weight ratio, (B) Lung DNA to protein ratio, (C) Lung DNA content normalized to lung weight, (D) Lung RNA content normalized to lung weight, and (E) Lung protein content normalized to lung weight. (F) Representative hematoxylin and eosin images of C57BL/6 E18.5 lungs without (scale bar = 50 µm) and (G) with fetal transuterine tracheal occlusion showing hyperplasia of conducting airways and increased size of distal airspaces; scale bar = 100 µm. Comparison of control (n=9) and tracheal occlusion (TO) (n=6) was performed using Student's t-test. Please click here to view a larger version of this figure.
| Table 1: Morphometrical results of groups | |||
| TO | Control | p | |
| Fetus weight (mg) | 1100.52 ± 229.38 | 1087.15 ± 172.32 | 0.896 |
| Lung weight (mg) | 28.41 ± 5.87 | 23.38 ± 3.09 | 0.043 |
| LBWR | 0.0259 ± 0.0021 | 0.0217 ± 0.0028 | 0.006* |
| Values expressed as means ± standard deviations. Abbreviations: LBWR = Lung to Fetal Body Weight Ratio; TO = tracheal occlusion. | |||
| *95% Confidence Interval 0.0222–0.0249. Groups compared by Student's t-test. | |||
Table 1: Morphometrical results of groups
