Source : Alexander Goldfarb, MD, professeur de médecine, Beth Israel Deaconess Medical Center, MA
Maladies gastro-intestinales représentent chaque année des millions de visites et d’admissions à l’hôpital. L’examen physique de l’abdomen est un outil essentiel dans le diagnostic des maladies de l’appareil digestif ; en outre, il peut aider à identifier des processus pathologiques dans les systèmes cardiovasculaires, urinaires et autres. L’examen physique en général, l’examen de la région abdominale est important pour établir un contact médecin-patient, pour aboutir au diagnostic préliminaire sélection ultérieure en laboratoire et tests d’imagerie et déterminer l’urgence des soins.
Comme avec les autres parties de l’examen physique, une inspection visuelle et l’auscultation de l’abdomen sont faites de façon systématique afin qu’aucun résultats potentiels ne sont manquées. Devrait être une attention particulière aux problèmes déjà identifiés par les antécédents du patient. Ici, nous supposons que le patient a déjà été identifié et a avait pris l’histoire, les symptômes discutés et secteurs préoccupants identifiés. Dans cette vidéo, nous n’examinerons pas les antécédents du patient ; au lieu de cela, nous irons directement à l’examen physique.
Avant de passer à l’examen, revoyons brièvement surfaces monuments de la région abdominale, anatomie abdominale et la topographie. Voici une liste des points de repère utiles : marges costales, processus xiphoïde, muscles abdominaux rectus, linea alba, ombilic, crête iliaque, ligament inguinal et la symphyse pubienne. L’examen abdominal étend vers le bas des marges xiphoid et costales supérieurement à la symphyse pubienne inférieurement.
À des fins diagnostiques et descriptives, l’abdomen est divisé en quatre quadrants : quadrant supérieur droit (souvent dénommée dans le QSD), laissa l’hypocondre (LUQ), quadrant inférieur droit (RLQ) et quadrant inférieur gauche (LLQ) (Figure 1). La topographie plus détaillée de l’abdomen divise en 9 régions : hypocondriaque droit et gauche, lombaire droite et gauche, droite et iliaque gauche et aussi des régions hypogastrique, ombilicales et épigastriques au milieu (Figure 2).
N’oubliez pas les organes en général du projet dans chaque région abdominale ()Figure 3). Il est essentiel de connaître l’anatomie de la région et la topographie bien de bien documenter et interpréter un patient plaintes et symptômes, ainsi que les signes physiques lors de l’examen.
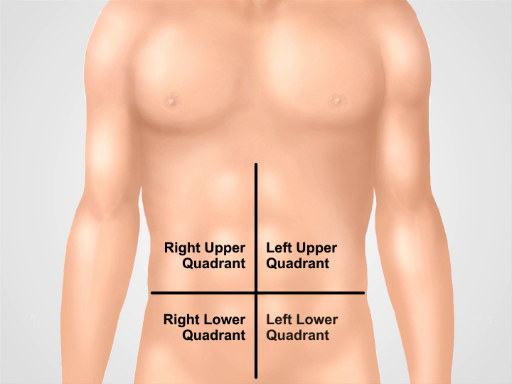
La figure 1. Quatre quadrants abdominaux. L’abdomen peut être divisé en quatre régions par deux lignes imaginaires qui se croisent à l’ombilic : quadrant supérieur droit (souvent dénommée dans le QSD), laissé l’hypocondre (LUQ), quadrant inférieur droit (RLQ) et gauche quadrant inférieur droit (LLQ) sont indiquées.
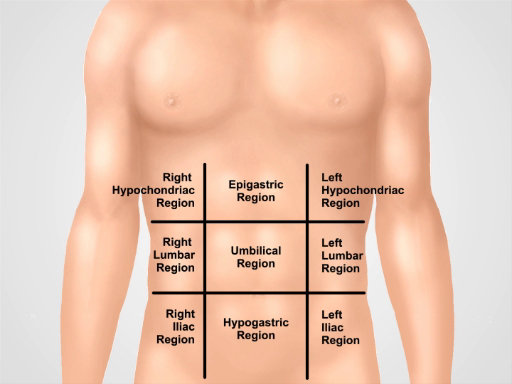
Figure 2. Neuf régions abdominales. Claviculaire lignes et plans sous-costales et intertubercular diviser l’abdomen en neuf régions : région épigastrique, région droite hypocondriaque, région hypocondriaque gauche, région ombilicale, région lombaire droite, région lombaire gauche, région hypogastrique, région inguinale droite et gauche région inguinale. Termes pour hypogastrique, ombilicale et épigastrique et régions sus-pubiennes sont les plus couramment utilisées en pratique clinique.
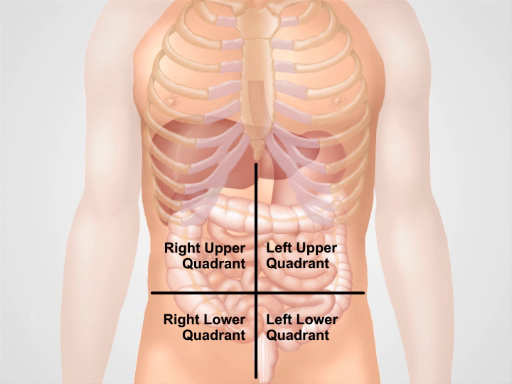
Figure 3. Localisation des différents organes dans les quatre régions abdominales. Organes dans la cavité abdominale et leur position en ce qui concerne les quatre quadrants abdominaux.