The capnography sampling lines used in these bench tests included 16 adult, pediatric, and neonatal capnography sampling lines from 7 commercial sources. Among the 16 sampling lines included in the bench tests, 5 sampling lines were from the same manufacturer as the capnography monitor utilized for the bench tests (‘matched’), and 11 sampling lines were from alternate manufacturers (‘cross-paired’) (Table of Materials). All of the nasal cannula sampling lines share a similar design, with up to 10 connection points between the cannula, humidifier, O2 connector, CO2 connector, 4-way, O2 tube, and CO2 tube (Figure 1).
1. Measure sampling line tensile strength
- Calibrate the tensile testing jig.
- In the tensile testing jig software, set the load cell selection to 100.00 kg and the load parameter to 10.00 kg.
- Attach sampling line components (example: O2 connector with O2 tube) to the calibrated tensile testing jig.
- Starting with a mass of 0 kg, initiate tension on the sampling line component and observe whether the sampling line connection remains intact.
- If the sampling line connection remains intact, automatically increase the mass in a continuous manner, and observe when the subparts break or disconnect.
NOTE: The resolution of the jig is limited to 10 g increments. - Record the maximum tension (kg) exerted before the sampling line break occurred.
- Repeat the tensile strength test for all 10 potential sampling line subparts: O2 connector with O2 tubing; O2 tubing with 4-way; 4-way with O2 tubing; O2 tubing with cannula; cannula with CO2 tubing; CO2 tubing with 4-way; 4-way with CO2 tubing; CO2 tubing with CO2 connector; humidifier with tubing; tubing with cannula.
- Repeat the tensile strength test on 16 sampling lines from 7 commercial sources.
2. Measure rise time and sampling line accuracy
- Calibrate the rise time measurement device.
- Cut standard 0.95 mm internal diameter CO2 PVC tube into ten 15 cm pieces.
- Operate the jig using the following steps:
- Turn on the air compressor, jig controller, and power supply.
- Open the CO2 gas flow.
- Attach the sampling channel directly to the measurement chamber without the sample.
- Calibrate the air and CO2 flow to 10 L/min and the gas sampling rate to 50 mL/min using a mass flow meter and a dedicated restrictor.
NOTE: The maximum sampling rate of the capnography monitor is 50 mL/min. - Open the jig software and define the test parameters as follows: Air:CO2 ratio 1:1; Air time = 3 seconds, CO2 time = 3 seconds, 10 cycles, rise time measurement length: none.
- Open the CO2 valve.
- Select the Finish Calibration button on the Measurement tab and make sure it turns green.
- Select the Measure button and wait for the gas flow cycles to end.
- Close the CO2 valve.
- Record the background rise time and ensure the result is less than 60 ms. If it is larger, clean the optical chamber with air flow and re-connect the y-piece/airway adapter properly.
- Take 10 measurements and calculate the average rise time value.
- Compare the rise time value to the margins and confirm it is inside the specification limits, pre-defined as rise time background < 60 ms and rise time of a control sample, a 15 cm PVC tube, 0.95 mm internal diameter, equal to 39 ± 5 ms.
- Compare the delivery time to the margins and confirm it is inside the specification limits, predefined as background delivery time <100 ms and delivery time of a control sample, a 15 cm PVC tube, 0.95 mm internal diameter, equal to 152 ± 5 ms.
- Open a new commercial sampling line.
- Connect the sampling line to the rise time measurement device.
- Click on the Start button in the rise time measurement device software and wait for the device to measure the rise time.
NOTE: The device repeats the measurement 10 times and automatically averages the repeats to report the rise time mean and standard deviation.- Copy the rise time result to the report.
- Disconnect the sampling line from the rise time measurement device.
- Calculate maximum respiratory rate for inhalation:exhalation time ratios of 1:1 and 1:2, in breaths per minute (BPM).
- Calculate the maximum respiratory rate using the measured rise time for the sampling line and a 1:1 breath ratio, using the following equation:

where 30 s represents the cumulative time used to exhale during 1 min (1:1 inhalation:exhalation time).
NOTE: For a 1:1 breath ratio, the maximum respiratory rate represents the fastest allowed respiratory rate without impacting ETCO2 accuracy when the time required for inhalation and exhalation is the same. - Calculate the maximum respiratory rate using the measured rise time for the sampling line and a 1:2 breath ratio, using the following equation:

where 40 s represents the cumulative time used to exhale during 1 min (1:2 inhalation:exhalation time).
NOTE: For a 1:2 breath ratio, the maximum respiratory rate represents the fastest allowed respiratory rate without impacting ETCO2 accuracy when the time used to exhale is twice as long as the time used to inhale.
- Calculate the maximum respiratory rate using the measured rise time for the sampling line and a 1:1 breath ratio, using the following equation:
- Calculate exhalation time for inhalation:exhalation time ratios of 1:1 and 1:2.
- For a 1:1 breath ratio, use the following equation:

where 30 s represents the cumulative time used to exhale during 1 min (1:1 inhalation:exhalation time). - For a 1:2 breath ratio, use the following equation:

where 40 s represents the cumulative time used to exhale during 1 min (1:2 inhalation:exhalation time).
- For a 1:1 breath ratio, use the following equation:
- Determine the accuracy of each sampling line at 150 BPM for 1:1 and 1:2 breath ratios by evaluating the maximum respiratory rate.
NOTE: If the maximum respiratory rate is ≥150 BPM, then the sampling line is considered accurate for the breath ratio, but if the maximum respiratory rate is <150 BPM, then the sampling line is not considered accurate at 150 BPM. - Repeat steps 2.2-2.8 for all 16 sampling lines tested.
- Perform statistical analysis using statistical software.
- Compare mean and standard deviation using Student’s t-test, with a two-sided significance level of 0.05, for all capnography monitor matched sampling lines vs. all capnography monitor cross-paired sampling lines.
- Repeat statistical analysis to compare all capnography monitor matched pediatric sampling lines to all capnography monitor cross-paired pediatric sampling lines.
- Repeat statistical analysis to compare all capnography monitor matched adult sampling lines to all capnography monitor cross-paired adult sampling lines.
3. Measure ETCO2 accuracy as a function of respiratory rate
- Prepare the manikin by placing in a supine position and connect the sampling line to the manikin per manufacturer instructions.
- Attach the sampling line to the capnography monitor and change the capnography monitor setting to accept sampling lines from all manufacturers by selecting Settings and Cancel Gold Ring Identification.
- Prepare and calibrate the breath simulator jig, to control the simulated respiratory rate.
NOTE: The breath simulator jig is composed of a 2-way electrical operating valve, allowing for precise control of the flow of CO2 and N2 to the manikin, to simulate human breathing.- Use a flow meter to measure the gas flow and calibrate it to 10 L/min.
- Open the breath simulator jig software and set the duty cycle to 50%.
- Test for leaks in the system using a leak testing jig.
- Connect the sampling line to the CO2 port on the leak testing jig.
- Create a kink in the sampling line to prevent CO2 from exiting the end of the sampling line.
- Using a flow rate of 50 mL/min CO2, allow the pressure in the sampling line to increase to 300 mmHg, and then stop adding CO2.
- Observe if the pressure in the sampling line remains the same or decreases. If the pressure decreases, this confirms a leak in the system, and a new sampling line should be applied in Step 4.2.
- Connect the breath simulator jig to the manikin.
- Increase the 5% CO2 flow rate to 10 L/min and the N2 flow rate to 10 L/min using the breath simulator jig. Keep flow rates constant throughout the test.
- Wait 30 seconds to allow a steady capnography waveform to be established, then record the ETCO2 value (mmHg).
- Measure a total of 10 ETCO2 values over 180 seconds.
- Change the respiration rate using the breath simulator jig, allow the capnography waveform to normalize for 30 seconds, and record 10 ETCO2 readings over 180 seconds.
- Repeat readings for each respiratory rate examined: 10, 20, 40, 60, 80, 100, 120, and 150 BPM.
- Determine the average and standard deviation of the 10 measured readings at each respiratory rate.
- Repeat steps 4.1-4.8 for all 16 sampling lines tested.
- Perform statistical analysis using Bland-Altman graphical plots to evaluate sampling line bias.
4. Measure ETCO2 accuracy in the presence of supplemental O2
- Prepare the manikin and breath simulator jig as described in Steps 4.1-4.3. Set the breath simulator jig to 10 BPM.
- Connect the O2 line to 100% O2.
- Increase the CO2 flow rate to 6 L/min and the O2 flow rate to 0 L/min, to use as a reference measurement.
- To allow the capnography waveform to stabilize, wait 30 seconds before recording the ETCO2 value.
- Read the ETCO2 value 10 times over 180 seconds.
- Change the flow rate of the CO2 and O2, allow the capnography waveform to normalize for 30 seconds, and repeat the 10 ETCO2 measurements over 180 seconds. To capture common clinical scenarios, use the following combinations of CO2 and O2 flow rates:
- Use a combination of 2 L/min CO2 and 2 L/min O2.
- Use a combination of 4 L/min CO2 and 2 L/min O2.
- Use a combination of 4 L/min CO2 with 4 L/min O2.
- Use a combination of 6 L/min CO2 with 4 L/min O2.
- Use a combination of 6 L/min CO2 with 6 L/min O2.
- Use a combination of 8 L/min CO2 with 6 L/min O2.
- Repeat the test as described in 5.1-5.6 for each sampling line.
- Perform statistical analysis using Bland-Altman graphical plots to evaluate sampling line bias.
Tensile strength
Sixteen capnography sampling lines from 7 manufacturers were tested to determine the tensile strength of each major sampling line joint (Figure 1, Table of Materials). Due to differences in sampling line design, not all joints exist in all sampling lines. The capnography monitor matched sampling lines 8, 9, 14, 15, and 16 had minimum overall tensile strengths between 3.55 kg and 5.94 kg. Most cross-paired sampling lines exhibited similar overall tensile strengths (Table 1). Sampling line 6 had the weakest tensile strength, with tensile strength equal to 1.33 kg at the connection between the CO2 tube and the 4-way. Common weak points among all sampling lines included the connection between the CO2 tubing and the 4-way, and the connection between the cannula and the CO2 tube.
Rise time
The rise time, defined as time required for the measured CO2 value to increase from 10% to 90% of the final value (Figure 2), was determined for the same 16 capnography sampling lines (Table of Materials). Comparison of capnography monitor matched vs cross-paired sampling lines found that the rise time for all cross-paired sampling lines was significantly higher (147 ± 23 ms vs. 201 ± 66 ms, respectively; p<0.001). A significant difference was also present between adult matched and cross-paired sampling lines (135 ± 13 ms vs. 214 ± 61 ms; p<0.001) but not between pediatric matched and cross-paired sampling lines (156 ± 25 ms vs. 169 ± 69 ms; p=0.395). Based on the measured rise time for each sampling line, the maximum respiratory rate (BPM), and exhalation time, using an inhalation: exhalation ratio of 1:1 and 1:2, the accuracy of each sampling line at 150 BPM was determined. While a majority of the sampling lines exhibited accuracy at 150 BPM for both breathing ratios, sampling lines 2, 3, 6, 7, 12, and 13 each failed to maintain accuracy at 150 BPM, whereas sampling lines 1, 4, 5, 8, 9, 10, 11, 14, 15, and 16 maintained accuracy in all tested conditions (Table 2). In particular, sampling lines 3, 6, and 13 all failed to meet the accuracy standard at 150 BPM in both the 1:1 and 1:2 inhalation:exhalation ratios.
ETCO2 accuracy as a function of respiratory rate
Accuracy of ETCO2 was measured using respiration rates between 10 and 150 BPM for 16 sampling lines from 7 manufacturers (Table of Materials). The expected ETCO2 in the presence of 5% CO2 was 34 mmHg at ambient pressure, and the range predefined as acceptable accuracy was ±2 mmHg for readings between 0-38 mmHg and ±5% of the reading + 0.08 for every 1 mmHg above 38 mmHg. Among the adult sampling lines tested, at 10 BPM, sampling lines 8 and 9 read ETCO2 equal to 33-34 mmHg (Figure 3A). Sampling lines 2, 5, 6, and 7 also read ETCO2 levels within an acceptable range (31-34 mmHg) at the lowest respiration rates (10-20 BPM). In contrast, sampling lines 3 and 4 reported low ETCO2 levels at the lowest respiration rate (10 BPM), and these readings decreased to 0 mmHg when the respiration rate increased to 80 BPM or higher. Only sampling lines 1, 8, and 9 continued to capture readings at very high respiration rates (120-150 BPM); sampling lines 2, 3, 4, 5, 6, and 7 read ETCO2 values equal to 0 mmHg at very high respiration rates (≥100 BPM). A similar pattern was observed in the pediatric and neonatal sampling lines, in which sampling lines 10, 11, 14, 15, and 16 captured readings across all respiration rates, and sampling lines 12 and 13 reported ETCO2 equal to 0 mmHg at respiration rates ≥100 BPM (Figure 3B). The bias of the ETCO2 readings was confirmed using Bland-Altman plots for capnography monitor matched and cross-paired sampling lines, where a majority of the ETCO2 measurements were within 95% limits, but the matched sampling lines exhibited higher accuracy with a bias toward overestimating ETCO2 at 150 BPM, and the cross-paired sampling lines strongly underestimated ETCO2 measures when respiratory rate was 80 BPM or higher (Figure 4A-B).
ETCO2 accuracy in the presence of supplemental oxygen
In addition to examining the accuracy of ETCO2 values of commercial sampling lines from 7 manufacturers (Table of Materials) as a function of respiratory rate, their accuracy was also evaluated in the presence of 2, 4, or 6 L/min supplemental oxygen (Figure 5), which represent the range of supplemental oxygen flow rates commonly used in clinical settings.3,29 In all cases, the expected ETCO2 was 34 mmHg. In the absence of supplemental oxygen, ETCO2 values were 34 ± 0 mmHg for sampling lines 8 and 9, and as low as 16 ± 0 mmHg for sampling lines 3, 4, and 12 (Figure 5A). Upon the addition of 2 L/min supplemental oxygen, a majority of sampling lines exhibited a decrease in observed ETCO2 values, ranging between 0 ± 0 mmHg and 23 ± 1 mmHg; sampling lines 7, 8, and 9 reported ETCO2 values between 33 ± 0 mmHg and 34 ± 0 mmHg (Figure 5B). The most extreme drop in ETCO2 value occurred in sampling line 2, which measured ETCO2 of 0 mmHg in the presence of as little as 2 L/min supplemental oxygen; this was also observed in sampling lines 2 and 5 in the presence of 4 and 6 L/min supplemental oxygen (Figure 5C-D). Decreased ETCO2 accuracy was also observed in sampling lines 1, 6, 10, 11, and 13 in the presence of 2, 4, or 6 L/min supplemental oxygen (Figure 5B-D). Bland-Altman plots for capnography monitor matched and cross-paired sampling lines indicate that while the matched sampling lines had high precision and limited bias in reading ETCO2 levels in the presence of supplemental oxygen, the cross-paired sampling lines consistently underestimated ETCO2 in the presence of supplemental oxygen (Figure 6A-B).
Table 1: Tensile strength test of capnography sampling lines. Please click here to download this table.
Table 2: Rise time for capnography sampling lines when used in conjunction with a portable capnography monitor. The rise time for each sampling line was measured 10 times to ensure accuracy of results. Please click here to download this table.
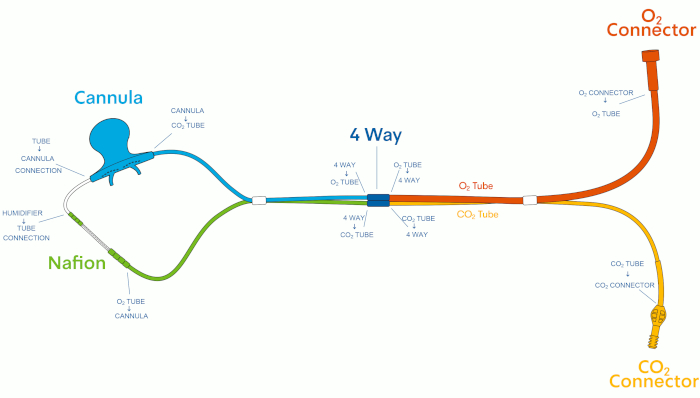
Figure 1: Capnography sampling line design. Please click here to view a larger version of this figure.
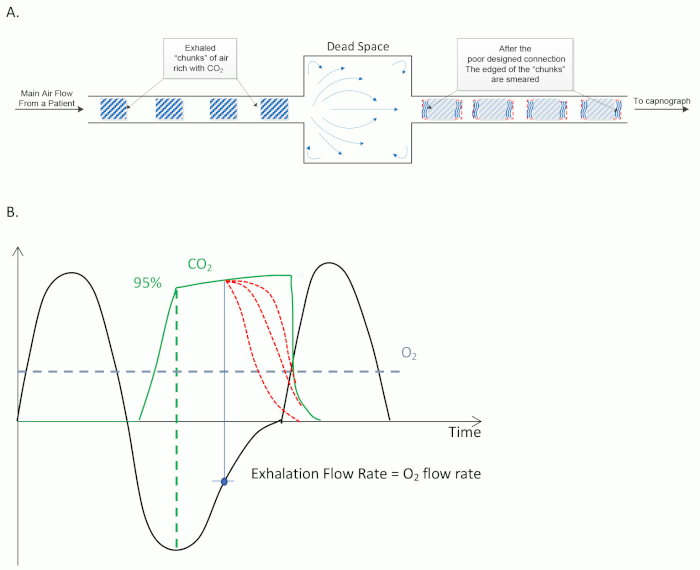
Figure 2: Fundamentals of sidestream capnography. (A) Example design of a sampling line, demonstrating how exhaled CO2 is sampled by the device. (B) Typical correlation between breathing flow rate (black line) and ETCO2 (green line) as function of time. A constant supplemental O2 flow is represented by a blue dashed line. Accurate measurement of ETCO2 occurs when CO2 has peaked (green dashed line). Inaccurate ETCO2 measurements (red dashed lines) can occur later in the breath cycle, when CO2 is diluted with supplemental O2. This occurs most often when the CO2 exhalation flow rate is equal to the flow of supplemental O2. Please click here to view a larger version of this figure.
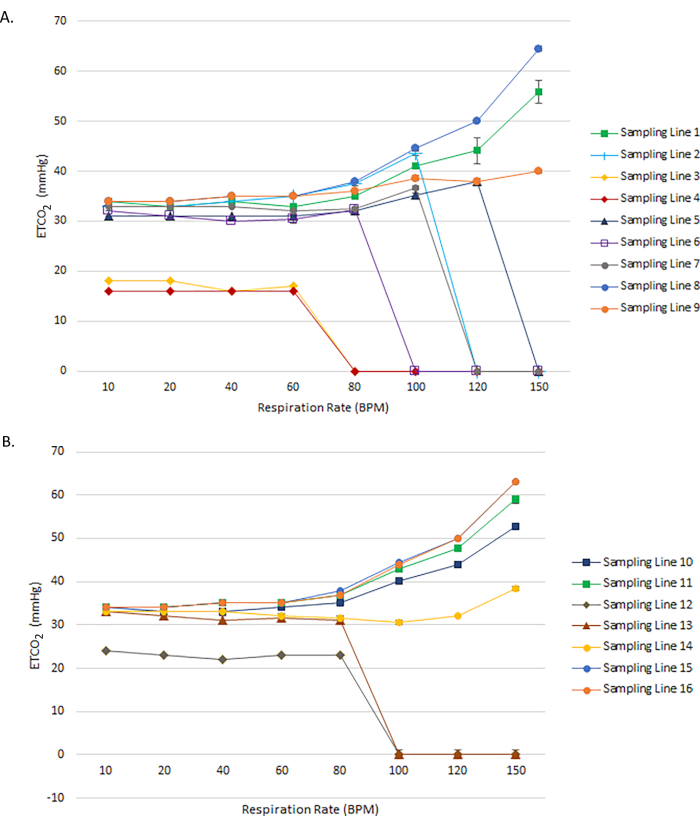
Figure 3: ETCO2 accuracy of adult and pediatric capnography sampling lines as a function of respiration rate. Measured ETCO2 values for (A) Adult and (B) Pediatric and Neonatal capnography sampling lines across a range of respiratory rates from 10 to 150 BPM. In all cases, the expected ETCO2 value is 34 mmHg. Please click here to view a larger version of this figure.
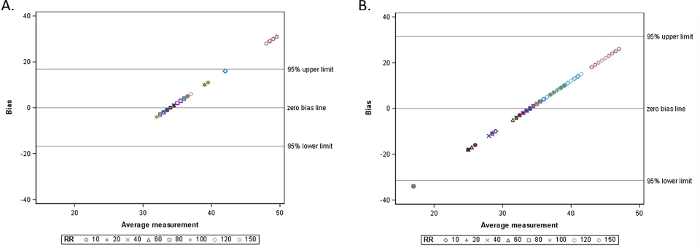
Figure 4: Bland-Altman plot for ETCO2 measures by (A) Matched sampling lines as a function of increasing respiratory rate and (B) Cross-paired sampling lines as a function of increasing respiratory rate. Please click here to view a larger version of this figure.
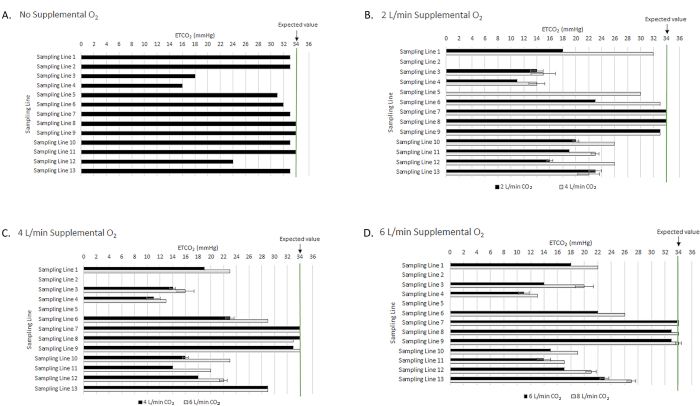
Figure 5: ETCO2 accuracy of capnography sampling lines in the presence of increasing supplemental oxygen. ETCO2 accuracy is reported for (A) No supplemental oxygen; (B) 2 L/min supplemental oxygen; (C) 4 L/min supplemental oxygen; and (D) 6 L/min supplemental oxygen. The green line at 34 mmHg represents the expected ETCO2 value across all measurements. Please click here to view a larger version of this figure.
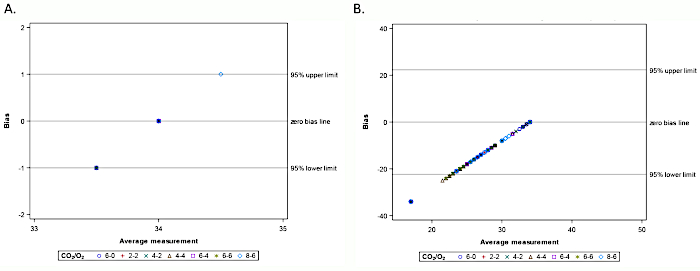
Figure 6: Bland-Altman plot for ETCO2 measures by (A) Matched sampling lines as a function of increasing supplemental O2 flow rate; (B) Cross-paired sampling lines as a function of increasing supplemental O2 flow rate. Please click here to view a larger version of this figure.
