In the representative case, the total operative time was 738 min, with an estimated blood loss of 400 mL. The patient was nursed in the intensive care unit for 2 days. The recovery was uneventful, and the patient was discharged on postoperative day 5. Histopathological examination of the specimen revealed moderately differentiated cholangiocarcinoma measured 8.0 cm x 5.5 cm x 4.5 cm. There was no perineural or lymphovascular permeation. The resection margin was 14 mm. The American Joint Committee on Cancer (AJCC) staging (8th edition) was pT1bN0M0. He was regularly followed up after the operation. The follow-up protocol is a 3-monthly follow-up in the first 2 years and then 6-monthly subsequently. The follow-up included clinical examination, liver function test and serum alpha-fetoprotein, and 6-monthly chest X-ray and contrast-enhanced computed tomography. All these details are listed in Table 1. The patient's first postoperative imaging is depicted in Figure 1C. It has been 2 years and 7 months post operation with no signs of recurrence and a normal serum alpha-fetoprotein level.
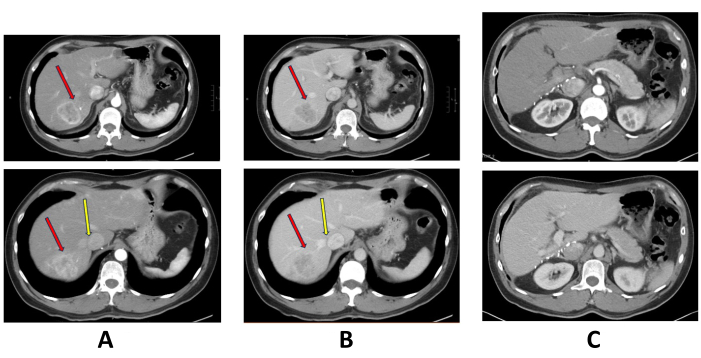
Figure 1: Pre-operative and postoperative triphasic computed tomography scan. (A) Arterial enhancing mass at segment 7 of the liver. The red arrow points at the tumor, and the yellow arrow points at the right hepatic vein. (B) The segment 7 tumor showed portovenous washout. The red arrow points at the tumor, and the yellow arrow points at the right hepatic vein. (C) Postoperative computed tomography scan. Please click here to view a larger version of this figure.
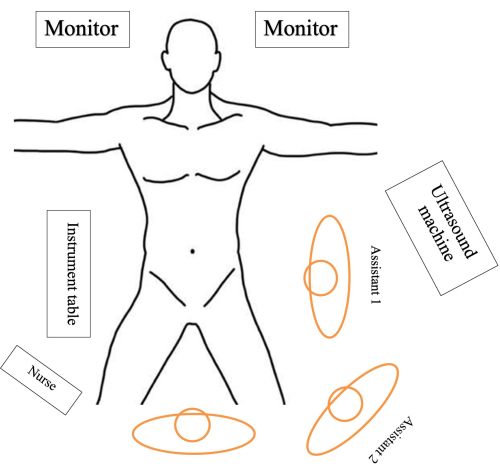
Figure 2. Patient positioning and theatre setup. The patient is placed in the Lloyd-Davis position on a split-leg table with the surgeon standing between the patient's leg. The first assistant stands on the patient's left side while the second assistant, responsible for holding the camera, stands between the surgeon and the first assistant. The instrumental table is placed on the right side while the scrub nurse standing next to the surgeon passes instruments to the surgeon. Please click here to view a larger version of this figure.
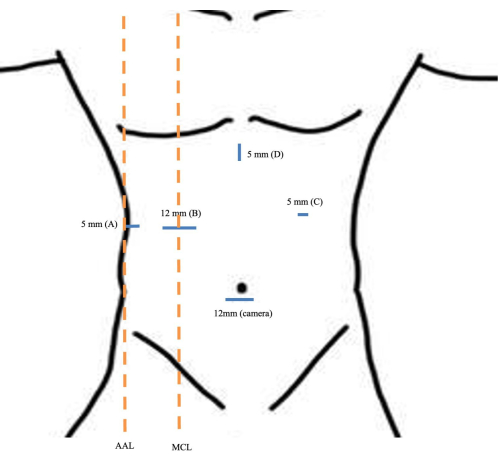
Figure 3. Port placement. 12 mm sub-umbilical port (camera port). (A) 5 mm port at the right flank along the anterior axillary line. (B) 12 mm port at the right upper quadrant along the mid-clavicular line. (C) 5 mm port at the left upper quadrant (liver retractor/assistant). (D) 5 mm port at epigastrium. Abbreviations: MCL = mid clavicular line; AAL = anterior axillary line. Please click here to view a larger version of this figure.

Figure 4. Flexible tip laparoscope. Its flexible tip (up-down and left-right) facilitates visualization of the anatomically obscured area, i.e., the dome. However, it requires a skillful and trained camera holder to operate this laparoscope21. Please click here to view a larger version of this figure.
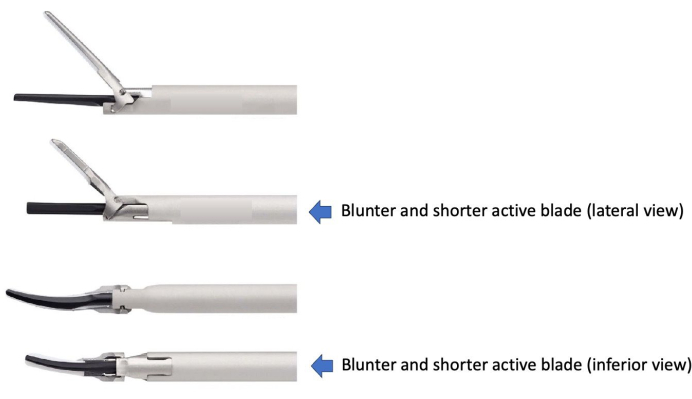
Figure 5. Difference between the two models of the ultrasonic scalpel. This figure has been modified with permission from Welling et al.22. Please click here to view a larger version of this figure.
| Total Operative Time | 738 min | ||
| Estimated blood loss | 400 mL | ||
| Day of discharge | Post-operative day 5 | ||
| Histopathological examination | Moderately differentiated cholangiocarcinoma | ||
| Size of tumour: 8.0 cm x 5.5 cm x 4.5 cm | |||
| Resection margin: 14 mm | |||
| No perineural or lymphovascular permeation | |||
| (American Joint Committee on Cancer (AJCC) staging (8th edition): pT1bN0M0) | |||
| First post-operative CT | See Figure 1C | ||
| Follow-up | Total follow-up period: 2 years 7 months | ||
| Status: No recurrence, normal serum alpha-fetoprotein level | |||
| Follow up protocol | |||
| · 3-monthly follow-up in first two years, then 6-monthly subsequently | |||
| · Clinical examination, liver function test and serum alpha-fetoprotein level, chest X-ray and contrast-enhanced computed tomography 6-monthly | |||
Table 1: Surgical outcomes and post operative details of the patient.
