Electrophysiological Measurement of Noxious-evoked Brain Activity in Neonates Using a Flat-tip Probe Coupled to Electroencephalography
Summary
Measuring pain in non-verbal patients is a challenge. In this study we combine EEG recording with stimulation using a flat-tip probe to detect noxious-evoked brain activity in an objective manner.
Abstract
Pain is an unpleasant sensory and emotional experience. In non-verbal patients, it is very difficult to measure pain, even with pain assessment tools. Those tools are subjective or determine secondary physiological indicators which also have certain limitations particularly when exploring the effectiveness of analgesia. As cortical processing is essential for pain perception, brain activity measures may provide a useful approach to assess pain in infants. Here we present a method to assess nociception with electrophysiological brain activity recordings optimized for the use in newborn infants. To produce highly standardized and reproducible noxious stimuli we applied mechanical stimulation with a flat-tip probe, e.g., PinPrick, which is not skin-breaking and does not cause behavioral distress. The noxious-evoked potential allows the objective measurement of nociception in non-verbal patients. This method can be used in newborn infants as early as 34 weeks of gestational age. Moreover, it could be applied in different situations such as measuring the efficacy of analgesic or anesthetic drugs.
Introduction
Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage1. The inability to communicate verbally does not negate the possibility that an individual is experiencing pain but makes it very challenging to assess pain-relieving treatment, for example in newborn infants2. Several behavioral and physiological indicators are used to assess pain in non-verbal patients. Different scales have been developed over the years, the choice depends on the type of stimulus, gestational age and the environment in which the neonates are embeded3,4,5. These pain assessment tools either rely on the rater's interpretation or they demand secondary physiological indicators.
In this video, we present a method to assess nociception with electrophysiological recordings optimized for use in newborn infants. Nociception is defined as the neural process of encoding noxious stimuli. Thus, quantitating nociception is an elegant and objective method to determine the neural input in a non-verbal person. Moreover, cortical activity detected by electroencephalography (EEG) is correlated with the intensity of noxious events5,6.
The method presented here combines EEG recording with noxious stimuli produced by a mechanical stimulation with a flat-tip probe, also called a pinprick7, which is not skin-breaking and does not cause behavioral distress6. It has been shown, that nociception following punctuate stimulation is predominantly mediated by Aδ-fibers, does not need a skin breaking lesion8 and the magnitude of the nociceptive-specific potential is not dependent on sleep state9. The probe is well accepted also by parents when applying this method in a study setting with neonates. The probe is electronically linked to the EEG recording system enabling the EEG recording to be precisely tagged when the probe contacts the skin. This greatly simplifies the process of time locking and is the premise for all subsequent EEG analyses. In order to minimize preparation time of the infant EEG recording we used a modified international 10/20 electrode placement system where we reduced the number of electrodes to the minimum requirement of three electrodes (Figure 1). The central vertex Cz electrode, where the noxious-evoked brain activity is maximal9,10,11, was used together with one reference and one ground electrode.
Protocol
The study was approved by the Competent Ethics Committee of Northwestern Switzerland (EKNZ 2015-079) and informed written parental consent for the participant was obtained before the measurement.
1. Preparation
- Make sure the baby is settled. It should be quiet and settled, without sucking motions during the recording because of movement artefacts. The baby can be asleep9.
- Measure the neonate's head circumference with a measuring tape to define the size of the EEG cap.
- Identify the active electrode position: Cz / vertex position by marking the middle point between nasion and inion and the middle point between the left and right preaurical point with a skin marker pencil. For positioning the electrodes see also Figure 1.
- Identify the positions of the ground electrode: right forehead (Fp2), and the reference electrode: left mastoid (A1).
- Clean the electrode sites (Cz, Fp2 and A1) with disinfectant using a cotton swab. In case of a lot of hair, separate the hair to visualize the scalp.
- Gently scrub the electrode sites with EEG prepping paste, using a cotton swab, to lower the impedance.
- Place the EEG cap with the electrodes attached on the neonate's head.
- Inject conductive EEG gel into the electrodes using a syringe with a short plastic needle to optimize the contact between the electrodes and the scalp.
- Adjust the electrodes until the impedance is below 50 kΩ as described in the manufacturer's recommendations and in published guidelines12.
- Position a camera to record the neonate's facial expressions.
- Connect the flat-tip probe to the contact trigger device, which is fixed to the EEG recording device. When the flat-tip probe reaches the nominal force on the skin, a trigger signal is generated by the contact trigger device. This signal is sent to the computer, tagging the EEG recording with a trigger mark.
2. Measurement
- Select a study name to store the data.
- Add online band pass filters:
- Display filters:
Low cutoff filter: Frequency: 1 Hz
High cutoff filter: Frequency: 70 Hz
Notch filter: 50 Hz
Sampling rate: 2000 Hz
- Display filters:
- Start the EEG and video recording.
- Hold the neonate's right hand in a horizontal position. The stimulus can also be applied on a different site, e.g. the foot, which will result in longer latency than from hand, please see for details 3.7.
- First record background EEG activity. Whilst the neonate's hand is held, annotate the EEG recording manually to record periods where no stimuli are applied and the infant is resting.
- Conduct the required amount of flat-tip probe stimuli according to the study design on the neonate's right hand. In our experimental design, set the the number of flat-tip probe stimuli at 50. Be careful to use the flat-tip probe perpendicularly to the neonate's hand so the tip does not bend and the correct force is applied. Perform the flat-tip probe stimuli using a minimum of a 2 to 3 s inter-stimulus interval (ISI)6 to avoid summation.
- Stop all the recordings.
- Document the experimental setting details.
3. Data Analysis
- Filter the raw EEG data offline using a high pass filter at 1 Hz and a low pass filter at 30 Hz.
- Segment the data in epochs of 1,500 ms (500 ms before to 1,000 ms after stimulus onset).
- Perform a baseline correction to the pre-stimulus interval.
- Manually reject the EEG epochs containing artefacts, such as movement artefacts and noise, after visual inspection. Please see also the tutorial outline: https://sccn.ucsd.edu/wiki/Chapter_01:_Rejecting_Artifacts
- Average the EEG epochs (for the background and stimulus response separately).
- Woody filter the data with a maximum jitter of ± 50 ms in the time window 0 – 1,000 ms post stimulus onset. This allows for latency differences between the infants. Do this for the background and stimulus responses separately.
- Project a template of noxious-evoked brain activity, that was defined in an independent dataset and has been described in detail elsewhere11 on to the data to ascertain the magnitude of the noxious-evoked response within each individual trial. The template describes a characteristic waveform of the noxious-evoked response and the magnitude reflects the amount of this noxious-evoked response within the individual trial.
NOTE: The time window on which to project the template is dependent on the age of the infant and the stimulus position. If stimuli are applied to the hand then the time window of interest is 200 – 500 ms post stimulus11. If the stimuli are applied to the foot then the time window of interest is 400 – 700 ms post stimulus11. Note that this template has only currently been validated for infants between 34 – 43 weeks' gestation. For detailed methods associated with using this template, and a discussion of the limitations, please see Hartley et al. 201711. - Check that the magnitude of the noxious-evoked brain activity calculated using the template is significantly higher following the stimulus, compared with in the background EEG.
- Analyze the behavioral facial expression afterwards (camera is linked to the EEG recording) using the Neonatal Facial Coding System2,13.
Representative Results
Figure 1 is the diagrammatic representation of the electrode positioning using the modified international 10/20 electrode placement system. Figure 2 shows the EEG activity recorded shortly before and after application of one single noxious stimulus using a flat-tip probe with 32 mN force, stimulation occurred as described in the protocol to the neonate's right hand (Figure 2A). The noxious-evoked response is visible at approximately 300 ms post stimulus onset (time 0). Figure 2B demonstrates the average response of 50 stimuli applied with a force of 32 mN to the same patient. Note that the noxious-evoked potential is more clearly if more stimuli are applied. Woody filtering, as shown in Figure 2C, can be used to adjust for slight variability in the response latency. The predefined template11, shown in red, is projected onto the EEG to calculate the magnitude of the noxious-evoked response.
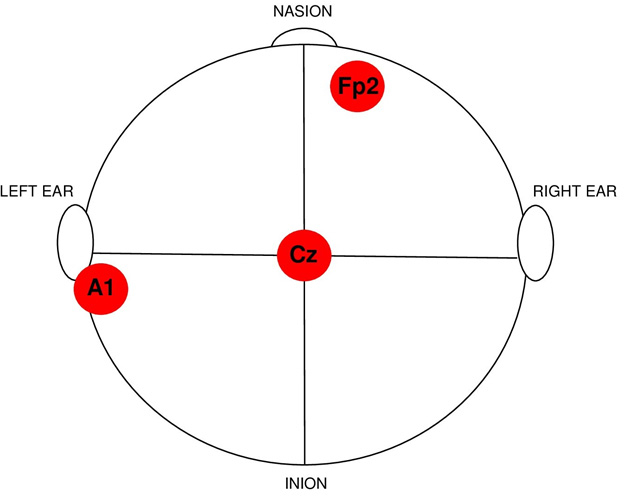
Figure 1: Diagrammatic representation of the electrode positioning using the modified international 10/20 electrode placement system.
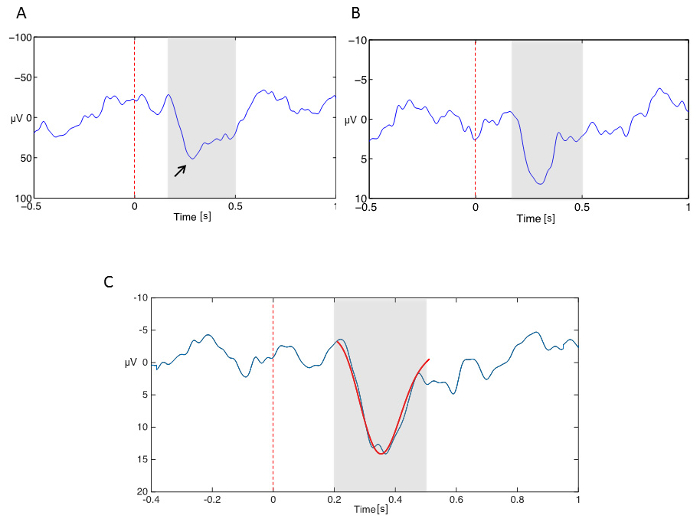
Figure 2: EEG activity recorded in response to the experimental noxious stimulation. A flat-tip probe stimulus (32 mN) was applied to the right hand of one patient, the time window of interest 200 – 500 ms after the stimulus is shaded. Panel A: EEG activity after one single stimulus, the principal peak at 250 ms is marked with an arrow. Panel B: Averaged response following 50 stimuli. Panel C: Woody filtered data with projected template (red). Please click here to view a larger version of this figure.
Discussion
The approach presented here shows how noxious-evoked brain activity in neonates can be measured in an objective way using EEG recording and flat-tip probe stimulators to apply experimental noxious stimuli. This technique can be used in various clinical settings to detect nociception, e.g. in non-verbal persons such as neonates. The complete study can be done within 15 min, including placing the baby, identifying, preparing and mounting the electrodes, and finally applying and recording the 50 noxious stimuli. The stimuli do not cause the infant behavioral distress, and this approach provides an objective method with which to assess nociception in infants.
In this study, we used a flat-tip probe stimulus with a mild force of 32 mN. Higher forces of 64 mN or 128 mN can also be applied in neonates but may lead to increased movements artefacts due to limb withdrawal. We noticed that in our study neonates accepted a force of 32 mN very well and did not withdraw their limbs, whereas a stimulus with 128 mN force leads to bilateral reflex withdrawal6. It has been shown that the noxious-evoked potential is greater depending on the force of the flat-tip probe stimulus (32 vs. 64 mN)6,14. Verriotis et al. showed that children at the age of 1 year have higher amplitude in their event-related vertex potential and higher pain scores than newborn infants15. Therefore, the force of the flat-tip probe stimulus can be adapted depending on the age of the patient16.
Previous studies recorded nociception from neonates being nursed supine or prone or even on their side. To keep experimental settings constant, we recommend keeping one position especially when performing a study with several participants. We found that performing the measurement in a supine position worked well. We performed the flat-tip probe stimuli on the neonate's hand. Positioning and handling of the neonate may be easier if applying the stimuli to the hand compared to the foot. The foot in fact is more commonly used in studies, however, we found that stimulating the back of the hand can be easier than accessing the foot. Reflex withdrawal is a useful additional measure of nociceptive activity, which can be incorporated into a multidimensional assessment of pain in this challenging non-verbal population17.
Despite avoiding any discomfort and movement artefacts there is always spontaneous neuronal activity. Thus filtering and averaging is important in order to attenuate the background noise and visualize the event related potential. Also, repetition of flat-tip probe stimuli, e.g. 50, strongly improves the signal-to-noise ratio. To analyze the data, time-locking of all the measurements is crucial.
A further technical challenge in neonates shortly after birth is the presence of vernix caseosa coating the skin of newborn infants including the head, which is why their skin needs to be cleaned carefully with an extra prepping paste even when active electrodes are used. In our opinion, active electrodes are better suited for this method than passive electrodes because they are less sensitive to external movement on the wires. Also, they are easier to use since they accept higher impedances due to the inbuilt pre-amplifier. However, passive electrodes can be used as well.
For data analysis, we used the method described by Hartley et al.6,11. Another method is the time-frequency analysis demonstrated by Hu et al.18.
Taken together, the technical methods, setup, and interpretation of the results require a trained team with preferably two people doing the measurement, one applying the stimuli while the other is checking the EEG. If the neonate is unsettled, the EEG will be contaminated with movement artifacts and it is not possible to perform the measurements. Also, because of validity, it is mandatory to have a certain number of stimuli, which can be challenging.
Nociception matures in early life and as early as 34 weeks' gestation the neonates' brain can distinguish between touch and nociception17. Under the age of 34 weeks' gestation infants are more likely to generate nonspecific neuronal bursts19 whereas in late-preterm infants starting at 34 weeks' gestation the here described method can be used11. This method opens the door for a variety of research investigations. For example, it could be used to test the impact of birth-related stress on nociception20 or to test the specific impact of various analgesic drugs in neonates and infants6,21. For example, the protocol presented here has been recently used in a study demonstrating the efficacy of topical local anesthetics in significantly reducing the noxious-evoked potential when a noxious stimulus was applied to a treated foot as compared to background activity or to the untreated foot11.
In conclusion, noxious-evoked brain potentials in EEG recordings make it possible to objectively investigate surrogate measures of pain perception in non-verbal patients. This method is applicable for use in the clinical setting in research investigations. By time-locking the flat-tip probe stimuli to the EEG recording it is possible to reliably evaluate the electrophysiological nociceptive response.
Declarações
The authors have nothing to disclose.
Acknowledgements
The authors would like to acknowledge Caroline Hartley and Rebeccah Slater (Department of Paediatrics, University of Oxford, UK) for critical reviewing our paper and Walter Magerl (Department of Neurophysiology, Center of Biomedicine and Medical Technology Mannheim (CBTM), University of Heidelberg, Germany) for supporting us with technical equipment and knowledge.
Materials
| Easycap | EASYCAP GmbH | AC-32-C | EEG caps for infants sizes 34 and 36 |
| actiCAP | Brain Products GmbH | BP-04243-SIG | active electrodes |
| ImpBox | Brain Products GmbH | impedance measurement | |
| V-Amp | Brain Products GmbH | EEG recording device | |
| Contact trigger for pinprick stimulation | MRC Systems GmbH | ||
| PinPrick stimulator set | MRC Systems GmbH | ||
| EEG prepping paste | USB Pharmacy | contains sodium chloride, pumice stone, propylene glycol | |
| SuperVisc | EASYCAP GmbH | Electrolyte-Gel for active electrodes | |
| Brain Vision Recorder | Brain Products GmbH | ||
| Brain Vision Analyzer | Brain Products GmbH | ||
| MATLAB using EEGLAB | Swartz Center for Computational Neuroscience, University of California San Diego | For EEG processing, including averaging of all EEG epochs |
Referências
- Bonica, J. J. The need of a taxonomy. Pain. 6 (3), 247-248 (1979).
- Duhn, L. J., Medves, J. M. A systematic integrative review of infant pain assessment tools. Adv Neonatal Care. 4 (3), 126-140 (2004).
- Witt, N., Coynor, S., Edwards, C., Bradshaw, H. A Guide to Pain Assessment and Management in the Neonate. Curr Emerg Hosp Med Rep. 4, 1-10 (2016).
- Hummel, P., van Dijk, M. Pain assessment: current status and challenges. Semin Fetal Neonatal Med. 11 (4), 237-245 (2006).
- Slater, R., Fitzgerald, M., Meek, J. Can cortical responses following noxious stimulation inform us about pain processing in neonates?. Semin Perinatol. 31 (5), 298-302 (2007).
- Hartley, C., et al. The relationship between nociceptive brain activity, spinal reflex withdrawal and behaviour in newborn infants. Sci Rep. , 31 (2015).
- Iannetti, G. D., Baumgärtner, U., Tracey, I., Treede, R. D., Magerl, W. Pinprick-evoked brain potentials: a novel tool to assess central sensitization of nociceptive pathways in humans. J Neurophysiol. 110 (5), 1107-1116 (2013).
- Ziegler, E. A., Magerl, W., Meyer, R. A., Treede, R. D. Secondary hyperalgesia to punctate mechanical stimuli. Central sensitization to A-fibre nociceptor input. Brain. 122 (Pt 12), 2245-2257 (1999).
- Slater, R., et al. Evoked potentials generated by noxious stimulation in the human infant brain. Eur J Pain. 14 (3), 321-326 (2010).
- Fabrizi, L., et al. A shift in sensory processing that enables the developing human brain to discriminate touch from pain. Curr Biol. 21 (18), 1552-1558 (2011).
- Hartley, C., et al. Nociceptive brain activity as a measure of analgesic efficacy in infants. Sci Transl Med. 9 (388), (2017).
- Keil, A., et al. Committee report: publication guidelines and recommendations for studies using electroencephalography and magnetoencephalography. Psychophysiology. 51 (1), 1-21 (2014).
- Grunau, R. V., Johnston, C. C., Craig, K. D. Neonatal facial and cry responses to invasive and non-invasive procedures. Pain. 42 (3), 295-305 (1990).
- van den Broeke, E. N., et al. Characterizing pinprick-evoked brain potentials before and after experimentally induced secondary hyperalgesia. J Neurophysiol. 114 (5), 2672-2681 (2015).
- Verriotis, M., et al. Cortical activity evoked by inoculation needle prick in infants up to one-year old. Pain. 156 (2), 222-230 (2015).
- Rolke, R., et al. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): standardized protocol and reference values. Pain. 123 (3), 231-243 (2006).
- Moultrie, F., Slater, R., Hartley, C. Improving the treatment of infant pain. Curr Opin Support Palliat Care. 11 (2), 112-117 (2017).
- Hu, L., Zhang, Z. G., Mouraux, A., Iannetti, G. D. Multiple linear regression to estimate time-frequency electrophysiological responses in single trials. Neuroimage. 111, 442-453 (2015).
- Hartley, C., et al. Changing Balance of Spinal Cord Excitability and Nociceptive Brain Activity in Early Human Development. Curr Biol. 26 (15), 1998-2002 (1998).
- Evers, K. S., Wellmann, S. Arginine Vasopressin and Copeptin in Perinatology. Front Pediatr. 4 (75), (2016).
- Slater, R., et al. Oral sucrose as an analgesic drug for procedural pain in newborn infants: a randomised controlled trial. Lancet. 376 (9748), 1225-1232 (2010).
