In this report, we present a novel ex vivo skin wounding and whole-mount staining approach to assess factors that influence the human skin repair response. Figure 1A shows a schematic of the procedural pipeline, which can be performed in 3-10 days, depending on wound incubation times. The partial thickness wounds are cultured on membrane stacks at the air : membrane interface and can be collected for whole-mount staining, embedded in paraffin or OCT medium for general histology, or frozen in liquid nitrogen for biochemical analysis (Figure 1B). We generally create 2 mm partial thickness wounds within the center of 6 mm explants. However, the size of the wound and surrounding explant may be altered depending on requirements. The whole-mount procedure has been successfully adapted for both immunoperoxidase and immunofluorescence staining methods (Figure 1C).
Immunofluorescence allows for the probing of tissue with multiple antibodies. For this, we advise using primary antibodies raised in different species, and species-matched fluorescently conjugated secondary antibodies to limit cross-species reactivity. Antibody concentrations and incubation times will need to be optimized. If background staining is observed, reduce antibody concentrations, increase wash steps, and add blocking buffer to the secondary antibody. Fresh tissue viability can be directly assessed with commercial viability dyes (see Table of Materials). We also show that tissue may be fixed post viability staining and successfully imaged when it is practically suitable (Figure 1D).
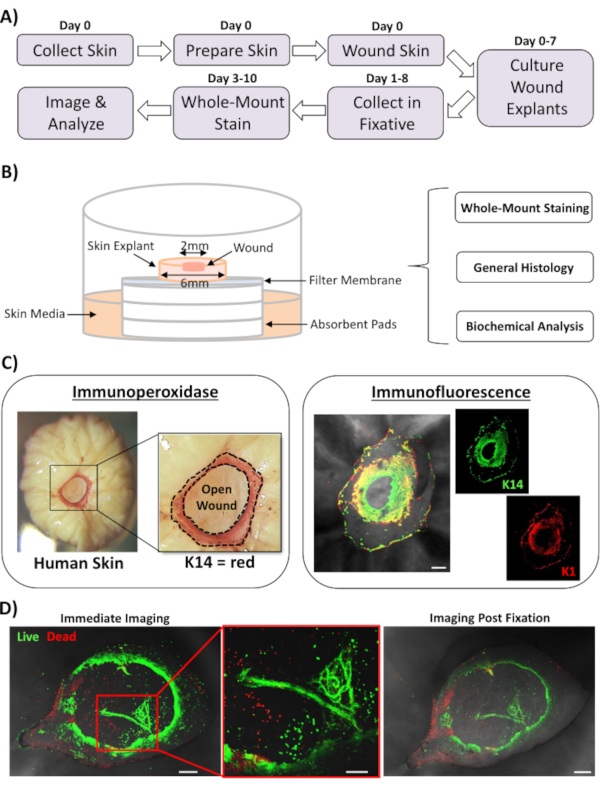
Figure 1: The human ex vivo wounding and whole-mount staining approach. (A) Pipeline depicting the procedural workflow from collecting skin and performing ex vivo wounding, to staining tissue and analyzing data. (B) Diagram demonstrating the human ex vivo skin wound culture system with analyses routinely performed on the tissue. (C) Whole-mount staining can be employed using both immunoperoxidase and immunofluorescence techniques. K14 = keratin 14. (D) Live tissue may be stained with commercial viability dyes and imaged successfully post fixation. Bar = 100 µm. This staining was performed in non-diabetic skin. Please click here to view a larger version of this figure.
The most widely applicable use for whole-mount staining of wounds is to determine wound closure rate in a more reproducible manner than can be provided via histological sectioning. Percentage closure was quantified as percentage re-epithelialization of the wound surface, as demonstrated in Figure 2A. Percentage area coverage of specific markers can be measured from the total wound area or as a percentage of the re-epithelialized wound. We characterized healing in healthy (non-diabetic) versus diabetic skin across a time course of seven days, collecting wounds at each day post-wounding (representative images, Figure 2B). Healthy skin wounds closed over time as expected, with full closure observed in most samples by day 4-5. On the contrary, diabetic skin wounds failed to close fully within the seven-day analysis period (Figure 2C). A significant delay in wound closure was observed between healthy and diabetic skin wounds when comparing healing rates at each time-point post-injury (P < 0.001 to day 6, P < 0.05 at day 6 and P < 0.05 to P < 0.001 at day 7).
Following assessment of overall wound closure rates; we measured the percentage of the entire wound area (outer area in Figure 2A) where K14 positive cells could be visualized (green staining in Figure 2B). Interestingly, we observed that in healthy ex vivo skin wounds, K14 staining peaked at day 2 and then rapidly declined (significance at each time-point versus the day 2 peak, Figure 2D). This is likely reflecting re-formation of the early epidermal barrier, excluding K14 antibody penetration through differentiated epidermal layers (see Figure 2E schematic). During the re-epithelialization process, basal layer (K14+ve) keratinocytes migrate inwards over the open wound such that the epidermis closer to the outer wound edge forms earlier than the epidermis closer to the inner wound edge (migrating front). While the front edge of the newly formed epidermis continues to migrate to close the remaining open wound, the outer edge epidermis begins to differentiate to reform the other epidermal layers. In early healing, we would thus expect to see most of the re-epithelialized area consists of basal (K14+ve) cells, while in later repair K14 staining is lost as the epidermis differentiates from the outside inwards (see whole-mount images in Figure 2E). Therefore, the decline in K14 staining shown in Figure 2D (downward arrows) correlates with increased epidermal differentiation. Interestingly, visible K14 staining peaked earlier in healthy (day 2) versus diabetic (day 4) wounds, further demonstrating that re-epithelialization and subsequent epidermal differentiation are delayed in diabetic skin wounds.
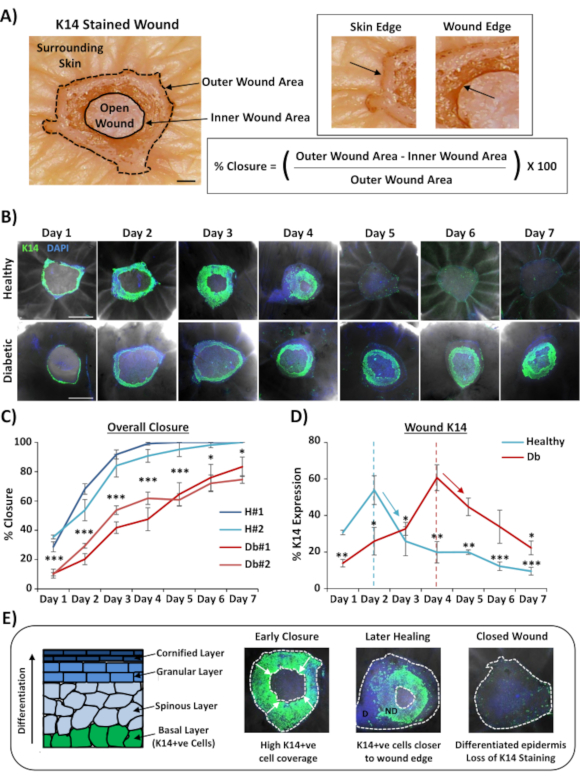
Figure 2: Whole-mount staining reveals perturbed healing rates in diabetic versus healthy skin. (A) The method used to quantify wound closure from outer and inner wound measurements. Brightfield images show keratin 14 (K14) staining in red. Bar = 300 µm. (B) Representative images of healing over time (day post-wounding) in healthy and diabetic skin. Bar = 500 µm. K14 = green. DAPI = blue nuclei. (C) Quantification of wound closure rates (percentage re-epithelialization) showing that ex vivo wounds from healthy skin close significantly faster than ex vivo wounds from diabetic skin. H = healthy. Db = diabetic. (D) Percentage K14 staining peaks earlier in healthy versus diabetic skin and then declines in line with increased epidermal differentiation (down arrows). (E) K14 (basal epidermal cell) staining is lost as the epidermis differentiates. D = differentiated. ND = not differentiated. White dotted lines depict inner and outer wound edges. White arrows = direction of migration. n = 6 wounds per donor, per time point. Mean +/- SEM. * = P < 0.05, ** = P < 0.01 and *** = P < 0.001. Healthy and diabetic compared at each healing time point in C (P value for least significant comparison). Temporal change in K14 staining compared to peak for each donor in D. Please click here to view a larger version of this figure.
We next used whole-mount staining to explore tissue expression and localization of other wound-relevant markers in non-diabetic skin (Figure 3). All antibodies used and their working concentrations are provided in the Table of Materials. Blood vessels in the open wound stained positively with alpha smooth muscle actin (a-SMA) antibody, used in combination with K14 to delineate the epidermal edges in lower power images (Figure 3A). The dermal matrix was stained with antibodies against collagen type I (COL 1) and fibronectin (Fn). Here collagen was observed as abundant thick fibers while fibronectin fibers were sparse, wavy, and thin (Figure 3A). Our whole-mount staining approach is also able to provide cell level resolution of staining, as demonstrated for K14-positive keratinocytes (Figure 3B).
Finally, we show that human ex vivo wounds possess resident immune cells, with Langerhans cells detected around newly formed epidermis at day 3 post-wounding (Figure 3C). Indeed, these results suggest that whole-mount staining may be used to investigate key features of the healing response including inflammation, proliferation, and the extracellular matrix (Figure 4A). Taken together, our data reveal that the combined ex vivo skin wounding and whole-mount staining procedure is a valid method to assess various aspects of healthy and diabetic (pathological) human skin repair.
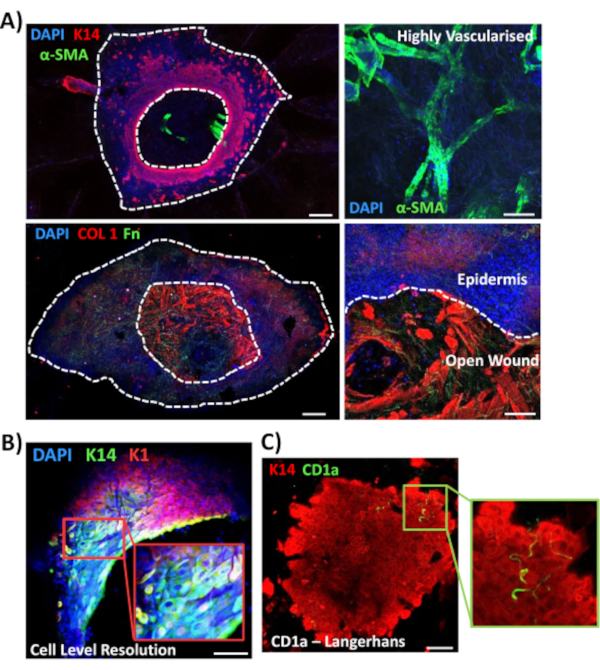
Figure 3: Optimization of the whole-mount staining approach for use with other antibodies. (A) Blood vessels were stained with alpha smooth muscle actin (α-SMA, green) and keratin 14 (K14, red), while matrix fibers were stained with collagen I (COL 1, red) and fibronectin (Fn, green). (B) The whole-mount procedure provides up to cell level resolution of localization (K14, green; K1, red). (C) CD1a+ve Langerhans cells (green) observed in newly formed epidermis. DAPI = blue nuclei. Bar = 100 µm. White dotted lines show inner and outer wound edges and separate wound from epidermis. This staining was performed in non-diabetic skin. Please click here to view a larger version of this figure.
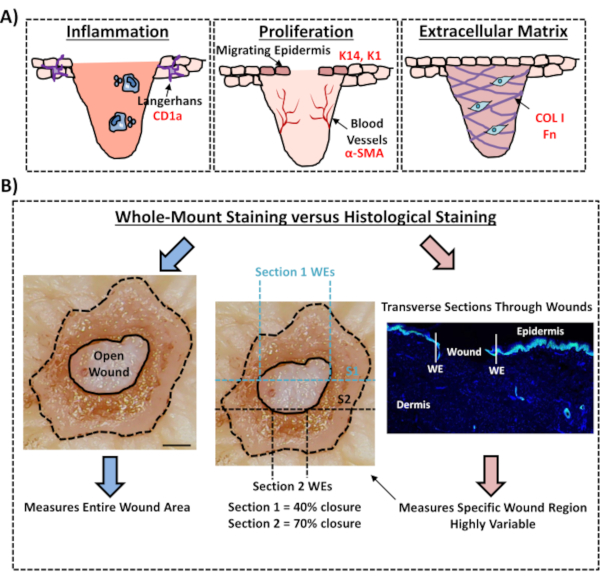
Figure 4: Validity of the whole-mount staining procedure for assessing wound healing. (A) Illustration depicting how the whole-mount staining technique can evaluate wound-relevant processes. Antibodies used = red text. K14 = keratin 14. COL 1 = collagen 1. Fn = fibronectin. (B) The whole-mount staining procedure (blue arrows) introduces less variability to wound closure measurements than standard histological analysis (red arrows). S1 = section 1. WE = wound edge. Bar = 300 µm. This staining was performed in non-diabetic skin. Please click here to view a larger version of this figure.
