Endolymphatic Duct Blockage as a Surgical Treatment Option for Ménière’s Disease
Summary
Endolymphatic duct blockage is a relatively new surgical method for patients suffering from Ménière’s disease. Following a regular mastoidectomy, the endolymphatic duct is identified and ligated using a regular titanium hemoclip. The effectiveness of this procedure is currently being assessed in a randomized trial.
Abstract
Endolymphatic duct blockage is a relatively new treatment option for Ménière’s disease, aiming to reduce vertigo attacks while sparing hearing and equilibrium. After a regular mastoidectomy, the posterior semicircular canal is identified, and Donaldson’s line is determined. This is a line through the horizontal semicircular canal, crossing the posterior semicircular canal. The endolymphatic sac is usually found at this site under the posterior semicircular canal. The bone of the endolymphatic sac and the dura are thinned until the sac is skeletonized, after which the endolymphatic duct is identified. The duct is then blocked with a titanium clip. Using a computerized tomography (CT) scan, the position is confirmed. Follow-up visits take place 1 week, 6 weeks and 1 year after surgery. To this day, only one prospective trial assessing this method has been conducted, comparing this new method to endolymphatic sac decompression. Results of the duct blockage are promising, with 96.5% of the patients free of vertigo after 2 years. However, further research is required.
Introduction
Ménière's disease (MD) is an incapacitating disease characterized by vertigo bouts, aural symptoms, and hearing loss1. Endolymphatic hydrops in the inner ear is present in patients with MD, but the exact aetiology of the disease remains unclear. In most patients, the symptoms resolve over time2; despite this, the majority of patients seek active treatment because of the unpredictable pattern of attacks.
Treatment for MD aims to reduce vertigo attacks. In the past century, different treatment modalities have been proposed, both surgical and non-surgical. Destructive surgical interventions, such as labyrinthectomy or vestibular neurotomy, are effective in controlling vertigo but cause deafness and a loss of vestibular function on the operated ear3,4. Surgeries on the endolymphatic sac (ES) have been studied, such as decompression and shunting of the sac, but neither of the proposed interventions have been proven to be more effective than placebo surgery4.
In 2015, Saliba et al. published the results of a randomized controlled trial comparing a new technique, endolymphatic duct blockage (EDB), to endolymphatic sac decompression (ESD)5. The trial yielded promising results, with 96.5% of the patients in the EDB group being free of vertigo attacks after 2 years. The rationale behind this technique is that the ES is at least partially responsible for the disturbed homeostasis of endolymph and produces an overload of endolymph due to increased production. By blocking the endolymphatic duct (ED), the surplus of endolymph that is generated in the sac is hindered from flowing to the rest of the inner ear. This hypothesis is supported by histological studies6,7,8.
Whether EDB is the appropriate treatment for an individual patient depends on various factors. The patient's preference and the surgeon's preference play a role, but local health care regulations may also influence treatment choice. In our center, EDB is only considered in patients who suffer vertigo attacks despite treatment with intratympanic (IT) injections with corticosteroids, and if vestibular migraine has been ruled out. EDB is especially suitable for patients with good hearing function who reject ablative treatment. This article describes the surgical steps of this new technique and discusses the literature that is currently available.
Protocol
This protocol is used for a randomized controlled trial that is currently being carried out in the Netherlands. The trial compares endolymphatic duct blockage (EDB) to endolymphatic sac decompression (ESD)9. The protocol was approved by the medical ethics committee METC Leiden-Den Haag-Delft (number P20.118) and the board of the hospital, as well as the hospital's research ethics committee (Haga Hospital Research Board, T20-108). All patients who participated in the trial where this protocol is followed have provided written informed consent. The results of this trial are expected in late 2024.
1. Preoperative procedures
- Patient selection
- Verify that all the diagnostic criteria for definite Meniere's disease according to the AAO-HNS criteria are met1. To be included in this study, select patients who have suffered more than three attacks in the previous 6 months. The attacks must meet the diagnostic criteria of an attack1.
- Rule out all the criteria of vestibular migraine reported by the consensus of the Bárány Society and the International Headache Society10.
- Due to its invasive nature, only consider this treatment in patients who have failed conservative treatment. This includes at least two intratympanic injections with (any type of) steroid and at least 6 weeks apart.
- In case of deafness of the contralateral ear, carefully consider this treatment option, as the effect of this surgery on hearing is not clear. This was reported to concern 2% of the patients by Saliba et al.5
- Informed consent
- Inform the patient about: potential benefits: reduction of vertigo attacks; risks: general risks of surgery (bleeding, wound infection, risks of general anesthesia), damage to the inner ear (deafness, disequilibrium), facial nerve damage, cerebrospinal fluid (CSF) leakage, and meningitis; and unknowns: effect on hearing loss, tinnitus, and aural fullness are currently unknown. The procedure seems to spare hearing function5,11, but the literature is limited.
- Preoperative testing
- Perform an MRI scan to rule out a retro-cochlear lesion, a CT scan, a hearing test (PTA), and electrocochleography preoperatively. Consider performing vestibular tests if the patient has complaints of chronic vertigo related to head movement.
- Check the CT scan for anomalies in the area of surgery, such as a high-riding jugular bulb. If a high-riding jugular bulb is present, this should be taken into account when operating. Also, assess the course of the vestibular aqueduct.
- Consider using an operation room that is equipped with a CT scan.
2. Operative procedures
- Setting up the operation room
- Place the anesthesia unit at the foot end of the patient to avoid problems with the CT scan.
- Place the control panel of the intraoperative neuromonitoring system as far away from the head of the patient as possible to avoid problems with the CT scan.
- Perform regular safety checks and induce general anesthesia.
- Using target-controlled anesthesia (TGA), administer propofol (2.5-4 mcg/mL) and remifentanil (0.3-0.5 mg/kg).
- Administer a low dose of the muscle relaxant rocuronium (0.3-0.5 mg/kg), as the facial nerve monitor is used during surgery.
- Intraoperatively, administer 4 mg of ondansetron and 4 mg of dexamethasone to prevent nausea postoperatively.
- Monitor the depth of anesthesia based upon hemodynamics-pulse, blood pressure, and CO2.
- Prepare analgesics to be administered at the end of surgery: 1 g of metamizole or 75 mg of diclofenac.
- Position the patient as for a mastoidectomy: rotate the head to the contralateral side (45° maximum) with the neck slightly in flexion.
- Preparation for surgery
- If necessary, shave any hair around the ear. Check to confirm if the tympanic membrane is intact.
- Sterilize the outer ear, the external ear canal, and the skin around the ear with chlorohexidine or povidone. Infiltrate the retro-auricular skin with 2% lidocaine/1:80,000 adrenaline.
- Cover the patient with sterile sheets, leaving the surgery area free.
- Surgery
- Make a retroauricular incision of 7-8 cm just behind the auricle using a scalpel. Spread the subcutaneous layers until the temporal muscle is visible at the cranial side.
- Make a Palva flap (anterior based) by making a U-shaped incision to the petrous bone. Be careful not to damage the temporal muscle.
- Using forceps and a raspatorium, peel the periosteum off the cortex until the external auditory canal is found.
- Position two spreaders in the tissue layers so that the petrous bone is exposed. Place the spreaders in a position such that their handles are away from the operation site.
- Perform a canal wall up mastoidectomy using the burrs. Form a triangle and burr through the cortex and identify the mastoid cells. Identify the sigmoid sinus (caudal) and dura (cranial) as landmarks.
- Identify the dura of the posterior fossa and the curvature of the horizontal vestibular canal. Identify the posterior semicircular canal (PSCC) and the dura mater of the posterior fossa.
- Identify the prominence of the horizontal semicircular canal (HSCC) to determine Donaldson's line, to approximate the position of the ES (see Figure 1).
- Thin the bone over the sac and the dura with diamond burrs and skeletonize the ES completely.
- Remove the remaining bone and expose the dura. Using an elevator, lift the dura toward the brain, exposing the medial side of the posterior canal. Identify the ES caudally as a flat, thick, white structure. The medialization of the dura exposes the ED somewhere in Donaldson's line, where it connects with the sacculus and utriculus.
NOTE: Be careful not to damage the duct. If the duct is damaged or ruptured, use fascia or donor pericardium to plug the leak. - Using the elevator, create a site to insert the tip of the instrument to clip the duct. At this level, in order to prevent any CSF leak, take care not to traumatize the dura, which is often thin.
- Using an elevator, try different clip sizes to determine which clip fits best.
NOTE: Thinning of the bone over the sigmoid sinus may be necessary to allow introduction of the clip instrument. - If a CT scan is available in the operation room, follow the subsequent steps.
- Without closing the clip, perform a CT scan. Cover the patient with a sterile cover. Position the scan so that the complete skull is scanned.
- Choose the protocol 20sDCT Head Micro under 3D head and follow the activate stand movements.
- Choose skull base and set up in the caudal-cranial direction. Follow the necessary 3D activate stand movement steps.
- After performing the scan, open Preset gallery and go to Head and neck. Select the preset DynaCTHead Petrosa.
- Assess the images to decide whether the clip is in the correct position. Do not forget to send the images to the patient file.
- If the clip is not placed correctly over the ED, replace the clip and/or consider using another size.
- Repeat step 2.5.12.2-2.5.12.6 of the CT-scan to assess the new clip position until satisfactory.
- Remove the clip with an elevator and place the clip in the clip applier. Place the clip over the ED and close the clip.
NOTE: Clipping of the duct causes traction on the involved structures and may lead to tearing of the dura. If CSF leakage occurs, use fibrin sealant and fascia or donor pericardia to close the tear in the dura. - Consider using a second clip to ensure the duct is tightly blocked. Ensure that the clips are positioned at the correct location and (completely) block the ED. If there is no CT scan available, check the clip position following the subsequent steps.
- Make an incision along the inferior edge of the ES, starting from the posterior site of the newly positioned clip toward the sigmoid sinus using a knife.
- If the incision opens the sac, this confirms the correct placement of the clip. If a CSF leak is observed, continue the dissection medially in order to localize the sac.
- Repeat this procedure until correct placement of the clip is confirmed.
- Completion of surgery
- Close the tissue in layers, close the Palva flap and the subcutaneous layer using an absorbable polyfilament suture (70 cm), and close the skin with an absorbable monofilament suture by applying a subcutaneous continuous suture (70 cm).
- Cover the closed skin with plasters and a bandage. Wrap one bandage around the head to keep the plasters in place.
- Administer the analgesic that was prepared in step 2.2.5.
3. Postoperative care
- Examination of the patient after surgery
- Determine if nystagmus is present. If spontaneous nystagmus is present, determine whether the fast phase is toward the operated ear or toward the contralateral side. If the fast phase is in the direction of the operated side, this indicates hyperexcitation of the operated ear and may be due to stimulation of the labyrinth from the surgery. This nystagmus is expected to fade out. If the fast phase is in the direction of the non-operated ear, this may indicate loss of function of the operated ear.
- Scratch the bandages to screen for loss of cochlear function. If the scratching on the operated side is not heard, and loss of hearing is suspected, consider administering steroids (1 mg/kg/day) for 7 days.
- Consider performing a bone conduction hearing on the day after surgery. If hearing loss is noticed, consider administering steroids (1 mg/kg/day) for 7 days.
- In case of pain, prescribe 1 g of acetaminophen (paracetamol) four times a day, and add 50 mg of diclofenac three times a day. In case of nausea, prescribe 4 mg of ondansetron.
- Keep the patient under observation until they are mobile, can eat and drink, and can go to the toilet independently.
- Consider dismissal on the day of surgery if the patient feels confident and has assistance at home. If the patient does not feel well, or feels dizzy or unbalanced, keep the patient overnight for observation.
- Upon dismissal, instruct the patient to keep the bandage around the head for 24 h, as well as the plasters underneath, keeping them dry until the next visit to the surgeon, 7 days after surgery.
- If bleeding or leakage of clear fluid occurs, ask the patient to contact the department immediately. In case of fever or excessive pain, ask the patient to contact the department.
- Explain what the patient can expect after the surgery-dizziness and vertigo attacks; dizziness and/or vertigo are common in the weeks after surgery. Inform the patient that having a vertigo attack does not mean that the surgery has failed. With regards to pain, most patients do not experience much pain after surgery, but acetaminophen (paracetamol) can be taken.
4. Postoperative visits
- Ask the patient to visit the surgeon 1 week after surgery. During this visit, remove the bandages and assess the wound. In case of signs of infection, prescribe antibiotics. In case of motion-related, short-lasting vertigo, consider that it might be benign paroxysmal positional vertigo (BPPV). Perform the Dix-Hallpike test, and if positive, carry out the Epley maneuver.
- Plan a PTA 6 weeks after surgery. Plan a follow-up visit 6 months and 1 year after surgery. Perform a hearing test at each visit.
Representative Results
Surgical factors
This procedure was performed by one of the authors (HB) in both the Haga Hospital and the Antwerp University Hospital. Data from the Antwerp University Hospital could not be retrieved, but approximately 100 patients underwent EDB at that location. In the Haga Hospital, EBD is only allowed in the context of the aforementioned trial. In this trial, surgery was performed on 38 patients. Due to the blinded character of the trial, it is unknown how many and which of these patients underwent EDB, and how many underwent endolymphatic sac decompression (ESD). However, these procedures are very similar and only differ in the closing or removal of the clip. Therefore, the surgery times are considered very similar, and we believe these are representative for EDB surgery. The mean time in the operation room (OR) was 132 min (standard deviation [SD]: 23 min; range: 90-194 min), and the mean surgery time was 97 min (SD: 22 min; range: 51-151 min). There was no noteworthy intraoperative blood loss.
Results of surgery
In 2019, patients who underwent EDB by one of the authors (HB) between 2015 and 2019 were asked to fill in two questionnaires postoperatively: the Ménière's disease outcome questionnaire (MDOQ) and a questionnaire about symptoms (vertigo, hearing loss, tinnitus, instability, and aural fullness). These results have been previously published9. The MDOQ is a questionnaire designed to evaluate surgical interventions for MD12. It results in two scores: one about the preoperative situation, and one about the postoperative situation. Each score can then be further divided into a score for the emotional, physical, and mental domain.
A total of 26 of the 42 operated patients agreed to participate. Patient characteristics can be found in Table 1. Of the patients (n = 23), 88% experienced a higher quality of life after EDB. None of the patients had a lower quality of life. Outcomes of the subjective complaints can be found in Figure 2.
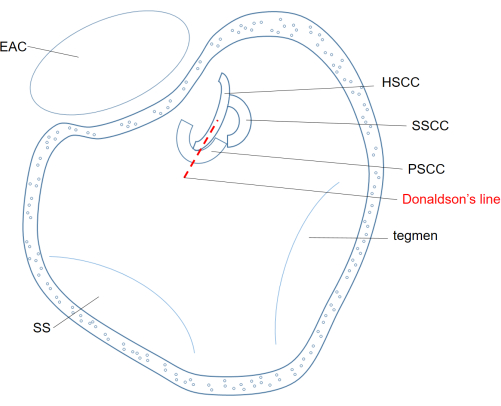
Figure 1: Mastoid after mastoidectomy in the left ear. Donaldson's line is projected over the (HSCC) and crosses the (PSCC). Following this line, the ES usually be found underneath the PSCC. Abbreviations: EAC = external auditory canal; SS = sigmoid sinus; HSCC = horizontal semicircular canal; PSCC = posterior semicircular canal; SSCC = superior semicircular canal. Please click here to view a larger version of this figure.
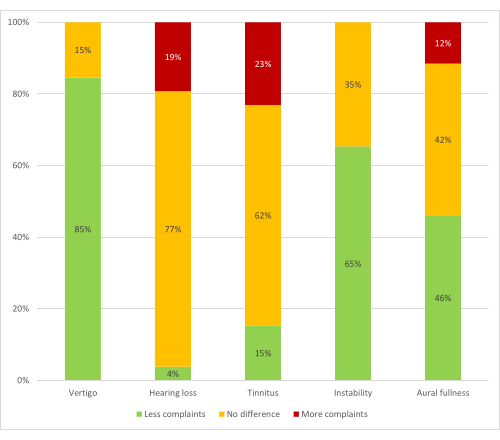
Figure 2: Outcomes of symptoms after EDB in 26 patients. X-axis: percentages of patients. Y-axis: complaints related to MD. Green columns: proportion of patients who experience less of the specific complaint; orange: proportion of patients who experience no difference regarding the specific complaints; red: proportion of patients who experience more of the specific complaint. Please click here to view a larger version of this figure.
| Age (years, mean) | 51 (SD 13) | ||
| Sex | Male | 12 | 46% |
| Female | 14 | 54% | |
| Side of Ménière's disease | AD | 8 | 31% |
| AS | 13 | 50% | |
| ADS | 5 | 19% | |
| Duration of Ménière's disease until EDB (years, mean) | 9.5 (SD 8.1) | ||
| Side of treatment | AD | 11 | 42% |
| AS | 14 | 54% | |
| ADS | 1 | 4% |
Table 1: Characteristics of patients who have undergone endolymphatic duct blockage, n = 42. Among these patients, there are slightly more females than males, and the left side was the most affected. AD = right ear, AS = left ear, ADS = left and right ear.
Discussion
EDB is a potential new treatment modality, aiming to reduce vertigo attacks while sparing inner ear function in patients with intractable MD. In the current literature, the results seem promising, but little data is available.
Rationale of the technique
Targeting the ES for relieving MD symptoms has been controversial for some decades. In the past, the general belief has been that the (ES) mainly has a role in the resorption of endolymph13,14,15,16. When the inner ear is separated from the ES where the endolymph is resorbed, this leads to hydrops. This hypothesis is supported by experiments performed on guinea pigs, in which blockage of the ED did indeed lead to hydrops in all the operated ears13. However, one should note that these experiments were performed on healthy guinea pig ears. Therefore, caution should be taken when extrapolating these results to human ears affected by MD. Consequently, the results of the paper by Kimura et al. do not necessarily refute the rationale of EDB in ears with MD. Furthermore, Lithicum et al. reported a case in which removal of the ES did not lead to an increase of hydrops17. This too refutes the theory that the ES is only a site of resorption of endolymph.
More recent literature endorses the hypothesis that the ES also has a role in production of endolymph, such as the demonstration of the presence of secretory (dark) cells in the ES7. Other histological studies confirm the production of endolymph in the ES, as well as hyperactivity at this site, leading to increased endolymph production6,8 . If the ES is responsible for the endolymph surplus, one may question why drainage of the ES has not been successful in relieving symptoms. However, the exact relationship between hydrops and symptoms remains enigmatic, and the resolving of hydrops does not seem pivotal to achieve a symptom-free state18,19.
Following from the arguments mentioned, we support the hypothesis that hyperexcitation of the ES causes an imbalance of the homeostasis of the inner ear, leading to the overproduction of endolymph, which then outweighs the resorption. By blocking the ED, this surplus is hindered from flowing to the rest of the inner ear.
Critical steps within the protocol
The site of the surgery, in the skull base, is reason for extra caution. Some critical steps in the protocol are described below.
Visualizing the anterior of the ED may be difficult, and estimating the size of the ED is necessary to be able to choose the correct clip size. A fish elevator can be used to palpate the anterior border of the ED if it cannot be visualized.
Vascular clip forceps are used to check the exposure of the ED. If the forceps fit, an open clip is placed, and a CT scan is made during surgery to check the clip position. If the clip is placed correctly, the open clip is removed, and one or two clips are placed using the forceps. Because the clip is placed, checked, removed, and then placed again, it poses a risk of misplacing the clip on the second occasion. In case of any doubt, another CT scan should be performed.
Skeletonizing the ED and closing the clip are critical steps in the procedure, as it causes traction on the dura and can therefore lead to CSF leakage. During skeletonizing and just after closing the clip, carefully check for CSF leakage. CSF leakage is repaired using a fibrin sealant, donor pericardium, and/or autologous fascia. A small tear is closed immediately with sealant, which is then supported with fascia. A larger tear should be managed carefully, to reduce the risk of later leakage and re-surgery. The suggested method to handle such a tear is to allow CSF to leak until the pressure has diminished, and then seal the leak with fibrin sealant and fascia. Check the site regularly for any leakage after repairing the tear. In case of a significant CSF leakage, a liquor drain and/or administration of acetazolamide (1 week, 250 mg twice a day), and/or a lumbal drain, can be considered.
Limitations of this method
As for every treatment modality for MD, it is important to realize that the pathophysiological mechanism of MD is not understood20. Therefore, it is difficult to determine what structure(s) should be targeted in the treatment. This technique targets the ES, but it has not been proven that this structure is responsible for the disease. Although the results so far are promising, the causal relation between surgery and reduced attacks cannot be proven. Therefore, physicians should realize that it cannot be determined whether this method targets the actual source of the disease or just induces a placebo effect.
Significance, importance, and potential applications
Many treatment options for MD, such as lifestyle adjustment, drugs, and intratympanic injections, have not proven to be effective or to only achieve temporary effects21,22,23,24. Moreover, surgical interventions are either not proven effective or cause irreversible damage to the inner ear4. EDB has the potential to fill the gap between these conservative methods and the destructive alternatives. However, the effectiveness is widely debated due to the lack of prospective, double-blinded studies assessing this method. An increase in knowledge on this topic could lead to an increase in the publication of data, and especially results, which could result in higher-quality levels of evidence. The application of the technique is currently limited to MD.
Declarações
The authors have nothing to disclose.
Acknowledgements
The authors thank Isobel Bowring for proofreading the article, and Nele Ruysschaert for the help with information on the anesthesia.
Materials
| Adson Forceps, Delicate, Smooth, 1 x 2 teeth, 12 0mm | Aesculap BV | BD511R | |
| Adson-Brown Tissue Forceps, 7 x 8 teeth, 120 mm | Aesculap BV | BD700R | |
| Baby Adson Retractor, hinged, semi-S tip, 3 x 4 prongs blade end, 140 mm | Aesculap BV | BV085R | |
| Baby Senn-Miller RetractorFlat Handle, SHARP tip, 3 PRONGS blade end, blade size 8 x 7/22 x 7, 165 mm | Aesculap BV | BT006R | |
| Bien Air Nano Micromotor OsseoDUO + NANOmicromotor | Bien air | 1700524-001 | Electronic motor used for mastoidectomy |
| Bien air tubing set for peristaltic pump | Bien air | 1100037 | |
| Coagulation Forceps | Aesculap BV | E700246 | Used for hemostasis |
| Cord, bipolar, 4.5 m | Valleylab BV | E360150L | |
| Diamond burrs 0.8x 70 to 7.0×70 | Bien air | ||
| Ear Curette, Pointed, Double Ended, cup size LARGE, 170 mm | Aseculap BV | OG189R | |
| Ethicon hechtdraad 3/0 sh-1 vicryl 70 cm | Ethicon | 3006273 | Suture for deeper tissue layers |
| Fibrin Sealant | Baxter BV | BE-90-01-040 | Tissue glue used in case of liquor leakage |
| Gillies Skin Hook, Tip 0.5/6mm, jaw STR, SERR | Aesculap BV | OL611R | |
| Gillies Tissue Forceps, Delicate, X-SERR tip, 1 x 2 teeth, 155 mm | Aesculap BV | BD660R | |
| Halsted Mosquito Forceps, Delicate, CVD jaw, 125 mm | Aesculap BV | BH111R | |
| Handpiece for burr | Bien air | 1600830-001 | |
| Hartmann Ear Forceps , Tip 4 mm, jaw STR | Aesculap BV | OG329R | |
| Hartmann-Wullstein Ear Forceps | Aesculap BV | OF410R | |
| Hejek Mallet, Ø27 220 mm | Aesculap BV | FL044R | |
| Horizon Metal Ligation System – Clips size MICRO, SMALL, MEDIUM | Teleflex Medical | 1201, 2200, 5200 | Titanium clip used for blockage of endolymphatic duct |
| House Ear Curette | Aesculap BV | OG182R | Double Ended, cup size (mm) 1.5/1.8, tip ANG |
| Lucae Bayonet Forceps | Aesculap BV | BD878R | SERR tip, 140mm |
| Lucae Bayonet Forceps | Aesculap | BD878R | SERR tip, 140mm |
| Lucae Ear Hook Button | Aesculap BV | OF278R | Hook end SMALL, tip SHARP, 130mm |
| Mayo Dissecting Scissors | Aesculap BV | BC587R | Round Blade, B/B tip, CVD blade, 165mm |
| Mayo Dissecting Scissors, Round Blade, B/B tip, CVD blade, 165 mm | Aesculap BV | BC587R | |
| McIndoe Thumb Forceps, Delicate | Aesculap BV | BD236R | SERR tip, 150 mm |
| Micro Adson Forceps, Delicate, SERR with platform tip Tip, 12 cm | Aesculap BV | BD220R/425.112 | |
| Monocryl 4-0 FS-2. 70 cm | Ethicon | Y422H | Suture for skin |
| NIM response 3.0 | Medtronic | NIM4CM01 | Nerve monitoring system |
| OSSEODUO control unit | Bien air | 1600513-001 | |
| Paired Subdermal electrodes with subdermal ground electrode and subdermal stim return, 2 channel | Medtronic Xomed | 8227410 | |
| Scalpel Handle #3 F/ Blades | Aesculap BV | BB070R | |
| Steel burrs 0.8x 70 to 7.0x 70 | Bien air | ||
| Volkmann Curette, tip size 3.6 mm, 170 mm | Aesculap BV | FK631R | |
| Watertight, 2-button multifunction pedal | Bien air | 1600517-001 | |
| Williger Bone Elevator, blade 6, 160 mm | Aesculap BV | FK300R | |
| Wire bending forceps, curved downards, 80 mm, jaw length 3.50 mm, with tubular shaft | McGee | OG359R | Used to close clip |
| Wullstein Retractor, sharp tip, 3 x 3 prongs blade end, 130 mm | Aesculap BV | BV076R |
Referências
- Lopez-Escamez, J. A., et al. Diagnostic criteria for Menière’s disease. Journal of Vestibular Research: Equilibrium & Orientation. 25 (1), 1-7 (2015).
- Perez-Garrigues, H., et al. Time course of episodes of definitive vertigo in Meniere’s disease. Archives of Otolaryngology-Head & Neck Surgery. 134 (11), 1149-1154 (2008).
- Alarcón, A. V., Hidalgo, L. O. V., Arévalo, R. J., Diaz, M. P. Labyrinthectomy and vestibular neurectomy for intractable vertiginous symptoms. International Archives of Otorhinolaryngology. 21 (2), 184-190 (2017).
- Pullens, B., Verschuur, H. P., van Benthem, P. P. Surgery for Ménière’s disease. Cochrane Database of Systematic Reviews. 2013 (2), (2013).
- Saliba, I., Gabra, N., Alzahrani, M., Berbiche, D. Endolymphatic duct blockage: a randomized controlled trial of a novel surgical technique for Ménière’s disease treatment. Otolaryngology-Head and Neck Surgery. 152 (1), 122-129 (2015).
- Møller, M. N., Kirkeby, S., Vikeså, J., Nielsen, F. C., Cayé-Thomasen, P. The human endolymphatic sac expresses natriuretic peptides. Laryngoscope. 127 (6), E201-E208 (2017).
- Takumida, M., Bagger-Sjöbäck, D., Wersäll, J., Rask-Andersen, H., Harada, Y. Three-dimensional ultrastructure of the endolymphatic sac. Archives of Oto-Rhino-Laryngology. 244 (2), 117-122 (1987).
- Friis, M., Thomsen, A. R., Poulsen, S. S., Qvortrup, K. Experimental hyperactivity of the endolymphatic sac. Audiology & Neuro-Otology. 18 (2), 125-133 (2013).
- Schenck, A. A., et al. Effectiveness of endolymphatic duct blockage versus endolymphatic sac decompression in patients with intractable Ménière’s disease: study protocol for a double-blinded, randomised controlled trial. BMJ Open. 11 (8), e054514 (2021).
- Lempert, T., et al. Vestibular migraine: Diagnostic criteria. Journal of Vestibular Research: Equilibrium & Orientation. 32 (1), 1-6 (2022).
- Schenck, A. A., Bommeljé, C. C., Kruyt, J. M. Outcomes of endolymphatic duct blockage for Ménière’s disease: an observational cohort study. American Journal of Otolaryngology and Head. 4 (5), 1140 (2021).
- Kato, B. M., LaRouere, M. J., Bojrab, D. I., Michaelides, E. M. Evaluating quality of life after endolymphatic sac surgery: The Ménière’s Disease Outcomes Questionnaire. Otology & Neurotology. 25 (3), 339-344 (2004).
- Kimura, R. S. Experimental blockage of the endolymphatic duct and sac and its effect on the inner ear of the guinea pig. A study on endolymphatic hydrops. The Annals of Otology, Rhinology, and Laryngology. 76 (3), 664-687 (1967).
- Lundquist, P. G. Aspects on endolymphatic sac morphology and function. Archives of Oto-Rhino-Laryngology. 212 (4), 231-240 (1976).
- Lundquist, P. G., Kimura, R., Wersaell, J. Experiments in endolymph circulation. Acta Oto-Laryngologica. Supplementum. 188, 198 (1964).
- Wackym, P. A., et al. Human endolymphatic sac: possible mechanisms of pressure regulation. The Journal of Laryngology and Otology. 101 (8), 768-779 (1987).
- Linthicum, F. H., Santos, F. Endolymphatic sac amputation without hydrops. Otology & Neurotology. 32 (2), e12-e13 (2011).
- Niu, Y., Chen, W., Lin, M., Sha, Y. Progression of endolymphatic hydrops and vertigo during treatment in Meniere’s disease. Acta Oto-Laryngologica. 142 (9-12), 653-657 (2022).
- Merchant, S. N., Adams, J. C., Nadol, J. B. Pathophysiology of Meniere’s syndrome: are symptoms caused by endolymphatic hydrops. Otology & Neurotology. 26 (1), 74-81 (2005).
- Basura, G. J., et al. Clinical practice guideline: Ménière’s disease. Otolaryngology-Head and Neck Surgery. 162, S1-S55 (2020).
- Hussain, K., Murdin, L., Schilder, A. G. M. Restriction of salt, caffeine and alcohol intake for the treatment of Ménière’s disease or syndrome. Cochrane Database of Systematic Reviews. 12, (2018).
- Burgess, A., Kundu, S. Diuretics for Ménière’s disease or syndrome. Cochrane Database of Systematic Reviews. 3, (2006).
- van Esch, B., et al. Betahistine for Menière’s disease or syndrome. Cochrane Database of Systematic Reviews. 1, (2001).
- Phillips, J. S., Westerberg, B. Intratympanic steroids for Ménière’s disease or syndrome. Cochrane Database of Systematic Reviews. 7, (2011).
