PV reconstruction is successful when, upon unclamping the portal vein, there is no tortuosity, and the liver is uniformly perfused. Anhepatic time should be under 20 min, as anhepatic times exceeding 25 min increase the risk of mouse mortality. IHIVC reconstruction is deemed successful if there is no blood regurgitation from the graft.
Storing the graft at cold temperatures for 1 h using organ preservation solution results in a serum alanine aminotransferase level of approximately 2,000 U/L at 6 h after reperfusion (Figure 7A). The survival rate is 100% at 7 days after transplantation (Figure 7B). However, in our model without hepatic artery anastomosis, recipient mice may succumb to intrahepatic biloma-related issues approximately 30 days post-transplantation
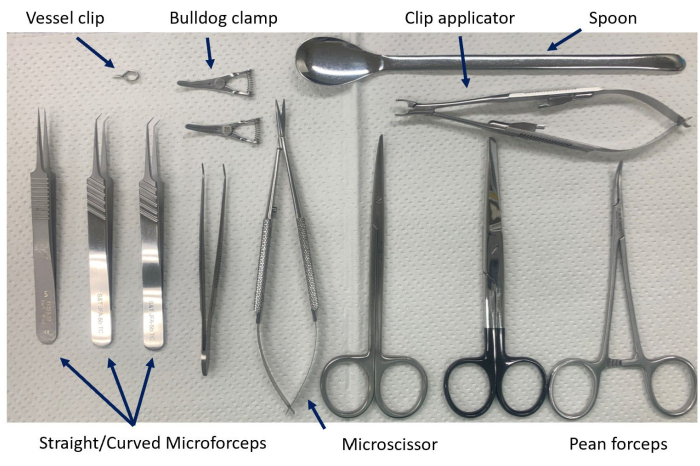
Figure 1: Instruments for vascular reconstruction. Straight or curved forceps are used as needed for the situation and the operative field. Please click here to view a larger version of this figure.
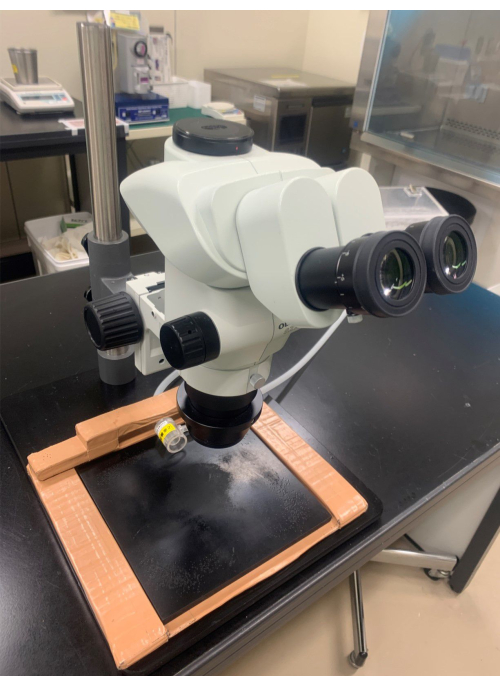
Figure 2: The microscope. The microscope is equipped with an objective lens with 10x magnification and an eyepiece lens with at least 0.8x magnification. Please click here to view a larger version of this figure.
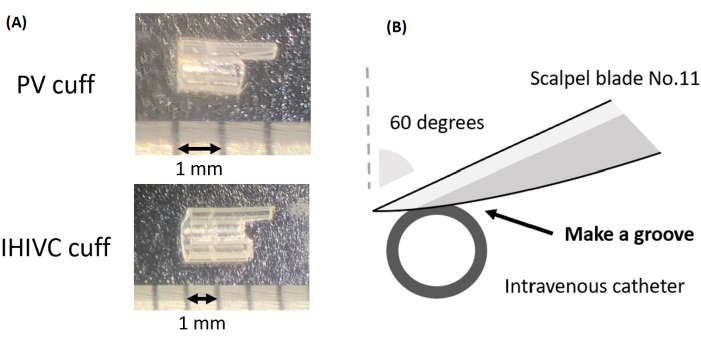
Figure 3: Preparation of the cuff. (A) The cuff for the PV and IHIVC. (B) A schematic representation of the process of creating a groove on the cuff. Please click here to view a larger version of this figure.
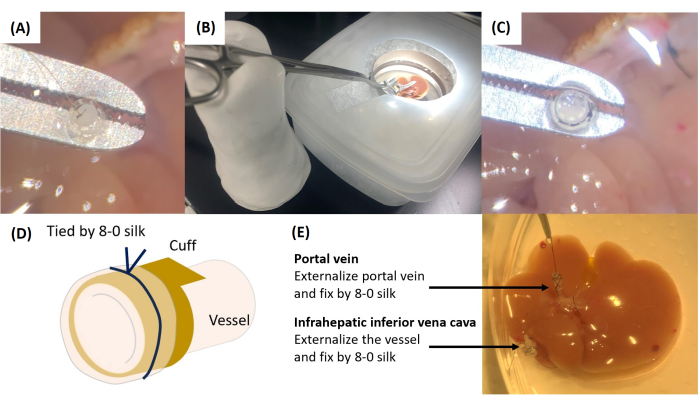
Figure 4: Cuff attachment. (A) The thread attached to the PV is passed into the cuff. (B) Instrument setup for cuff attachment. (C) Securing the cuff with 8-0 silk ligations. (D) Schematic illustration of vascular externalization and fixation to the cuff. (E) Completed cuff attachment. Please click here to view a larger version of this figure.
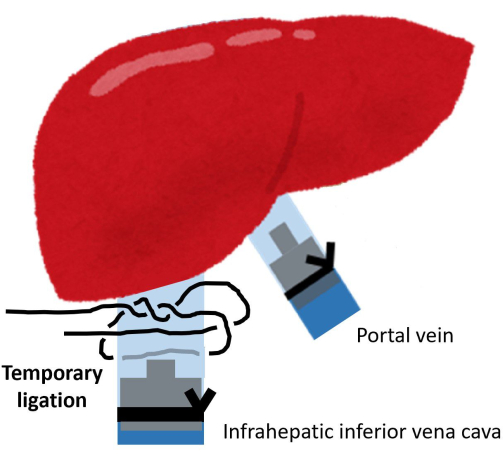
Figure 5: Temporary ligation of the IHIVC root. Please click here to view a larger version of this figure.
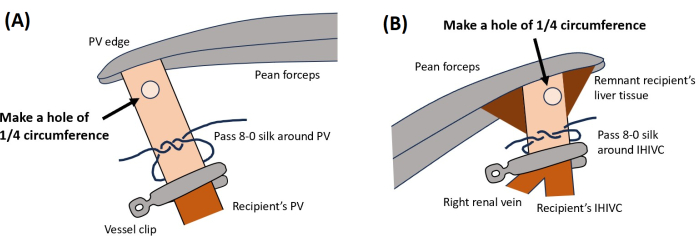
Figure 6: Vascular reconstruction. This illustration shows the locations for creating holes for (A) PV and (B) IHIVC. Please click here to view a larger version of this figure.
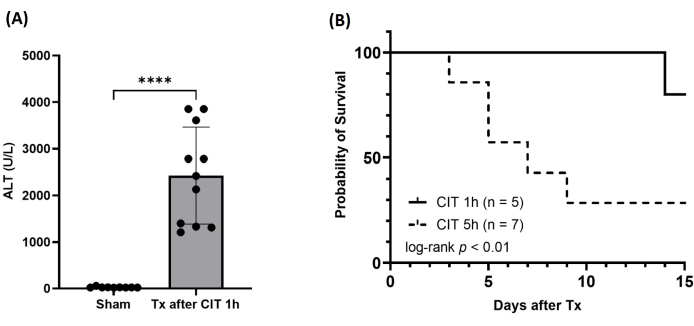
Figure 7: Postoperative results. (A) Serum levels of alanine aminotransferase (ALT) at 6 h after reperfusion. CIT, cold ischemic time; Tx, transplantation. ****p < 0.0001. (B) Survival of the recipient after MOLT. Please click here to view a larger version of this figure.
