Operation characteristics
The surgical navigation system was applied in continuative 10 hips of nine patients. The average total positioning time of the surgery was 10.1 min (median 9.5 min, range 8.0-14.0 min). The mean C-ARM fluoroscopies was 5.5 times (median 5.5 times, range 4-8 times). The mean error of puncture accuracy was 1.61 mm (median 1.2 mm, range -5.76-19.73 mm; Table 1). The results show that the positioning time and fluoroscopy times are obviously shortened compared to traditional procedures.
Clinical outcome evaluation
The nine enrolled patients consisted of seven males and two females, with an average age of 41.6 ± 10.0 years.The mean BMI was 23.93 ± 3.08 kg/m2. For the hips evaluated, two hips were in ARCO I stage, four hips were in ARCO IIA stage, and four in ARCO IIB stage. Preoperative and postoperative visual analogue scale and Harris hip score were used to evaluate the outcome (Table 1). The mean preoperative VAS score was 6 and mean postoperative score was 3.75. The average preoperative Harris score was 77.5 and mean postoperative score was 85.5. Hip X-ray was examined 3 months after the surgery. All the patients returned to the ward safely. No postoperative complications such as infection, hematoma, or nerve damage were found. So far, no femoral head collapse occurred in any cases, and the long-term function and success rate of hip preservation are still being followed up. Surgical indicators and scores are shown in Table 2.

Figure 1: Imaging of early stage of femoral head necrosis. (A) The CT image. (B) The MRI image. Arrows indicate areas of necrosis. Please click here to view a larger version of this figure.
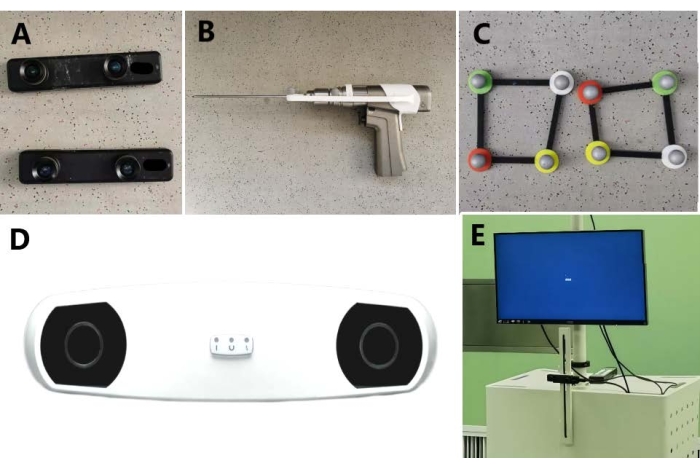
Figure 2: The main components of the AR-based navigation surgical system. (A) Depth camera. (B) The puncture device with a positioning frame. (C) Non-invasive body surface marking frame independently designed and developed. (D) Infrared positioning device. (E) The surgical system workstation. Please click here to view a larger version of this figure.
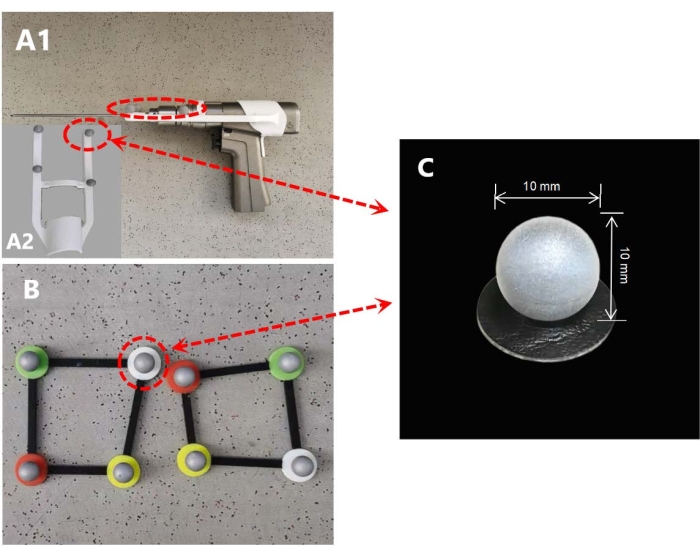
Figure 3: Installation of a passive infrared reflector. (A) Self-designed positioning frame mounted on puncture device. (B) The reflector is mounted at the four corners of the non-invasive body surface marking frame. (C) The specification of the passive infrared reflector is a spherical device with a diameter of 10 mm. Please click here to view a larger version of this figure.
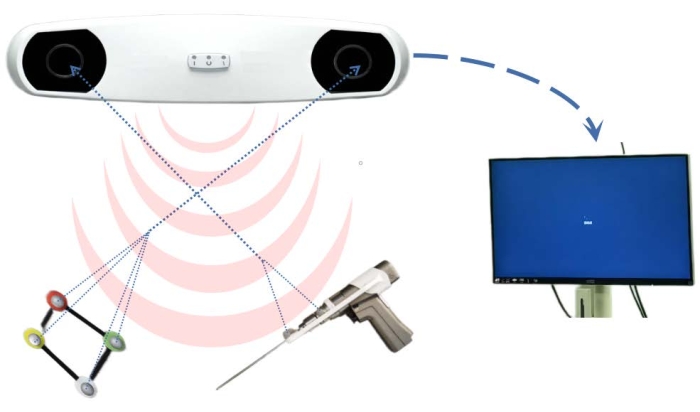
Figure 4: Working principles of infrared positioning device. Infrared radiation emitted by the infrared positioning device is reflected by the passive infrared reflectors; the receivers in that device receive the reflected signal and transmit the movement data to the workstation. Please click here to view a larger version of this figure.
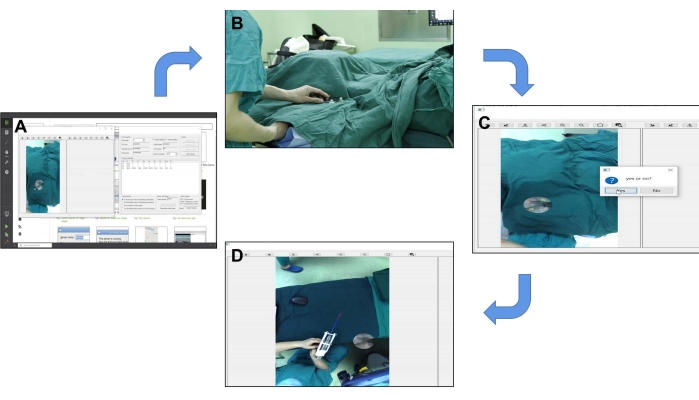
Figure 5: An overview of the preoperative registration process. (A) Operating interface of AR-assisted orthopedic surgery system. (B) The surgical area was planned using a non-invasive body surface marking frame. (C) Tips for successful registration of one of the matching points in the surgical video. (D) After all the matching points were successfully matched, the tracking of surgical instruments was tested. Please click here to view a larger version of this figure.
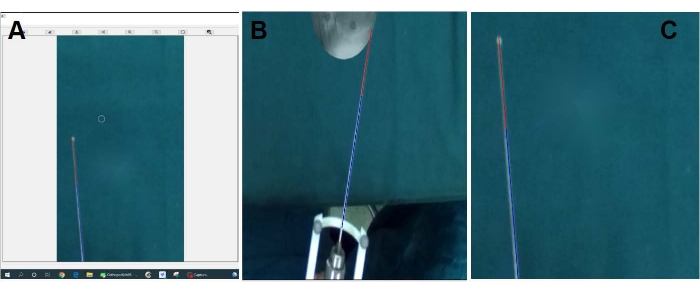
Figure 6: Superposition of virtual Kirschner wire on real Kirschner wire. (A-C) The images show that the virtual Kirschner needle is precisely superimposed on the physical one and moves with it in the screen. Please click here to view a larger version of this figure.
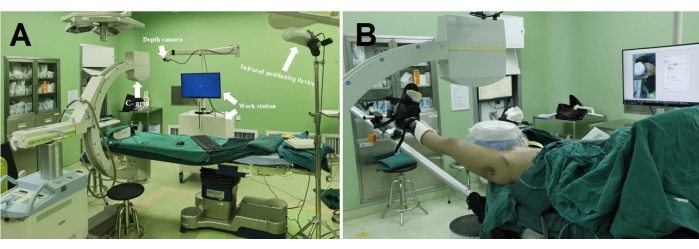
Figure 7: An overview of surgical scenarios. (A) The main components of the AR-based surgical system in the operating room. (B) A patient with necrosis of the femoral head is being treated with the aid of the surgical system. Please click here to view a larger version of this figure.
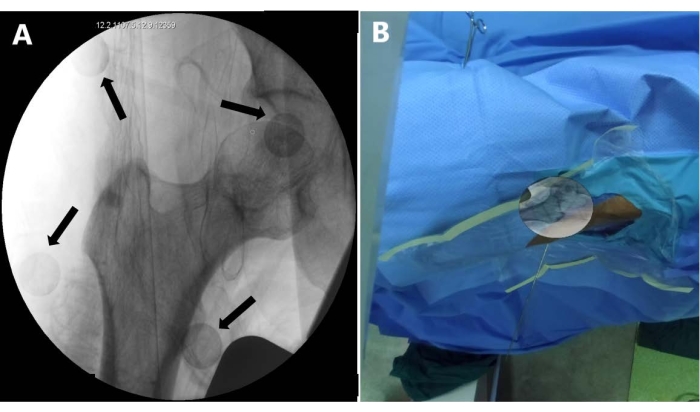
Figure 8: Hip joint imaging and augmented reality display. (A) Radiograph of the hip joint containing a non-invasive body surface marking frame. The black arrow indicates the passive infrared reflectors. (B) Radiograph is processed at the workstation and then superimposed by the surgical system on the surface of the affected hip on the screen. Please click here to view a larger version of this figure.
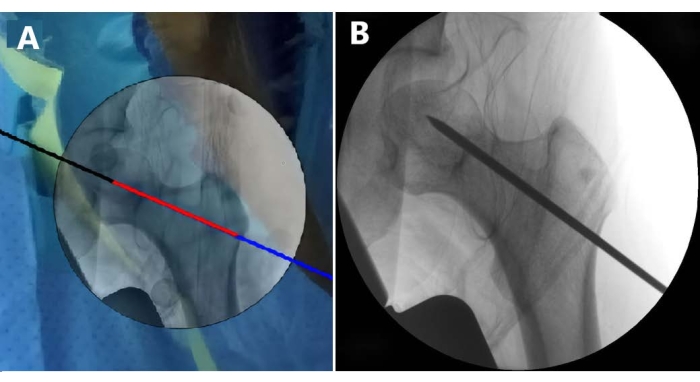
Figure 9: Puncture effect demonstration. (A) Image presents the screenshot after the puncture, the black-red-blue line is a virtual Kirschner wire in the system (step 2.6). (B) Image shows the hip radiograph after completion of puncture, the black line is an image of a real Kirschner wire in X-ray. Please click here to view a larger version of this figure.
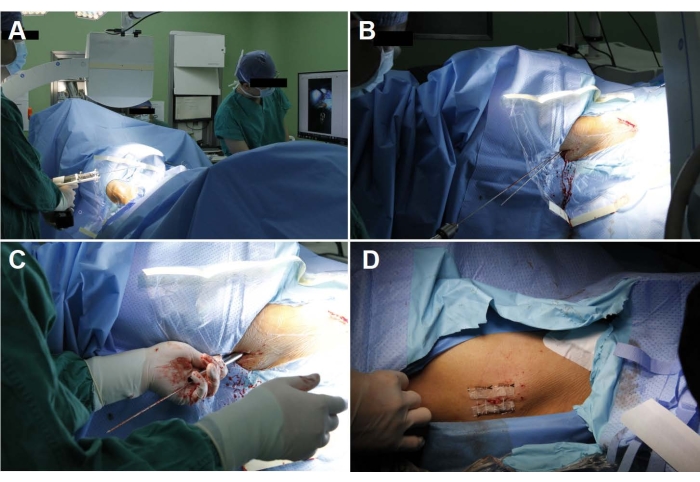
Figure 10: Femoral head puncture guided by the AR-based surgical system. (A) The surgeon is adjusting the position of the puncture device according to the screen display. (B) Kirschner wire punctures the skin and points to the necrosis. (C) Drill into the necrotic area along the Kirschner wire with a 5 mm trephine to fill artificial bone or autologous bone implantation. (D) Close the wound. Please click here to view a larger version of this figure.
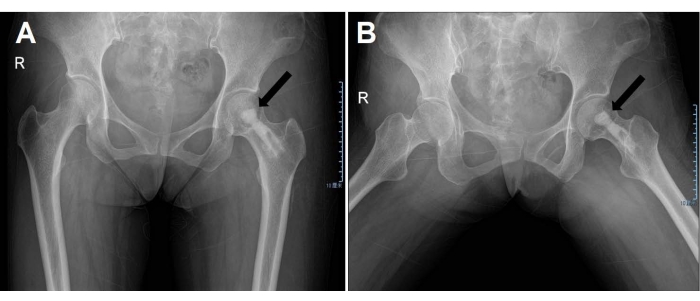
Figure 11: Postoperative radiograph of the hip joint. (A) From the front view. (B) The patient is in frog position. The black arrows indicate artificial bone implants in the femoral head. Please click here to view a larger version of this figure.
| Case | Sex | Age | BMI | Disease | ARCO |
| 1 | M | 22 | 28.40 | ONFH(left) | IIA |
| 2 | F | 21 | 22.40 | ONFH(right) | IIB |
| 3 | M | 42 | 19.56 | ONFH(left) | IIB |
| 4 | M | 51 | 22.10 | ONFH(left) | I |
| 5 | M | 31 | 24.34 | ONFH(bilateral) | L:IIB |
| 6 | R:IIA | ||||
| 7 | M | 46 | 27.24 | ONFH(right) | IIA |
| 8 | F | 41 | 21.20 | ONFH(left) | IIB |
| 9 | M | 56 | 22.83 | ONFH(right) | I |
| 10 | M | 38 | 27.30 | ONFH(left) | IIA |
Table 1: Basic patient information. The table provides the information for the 10 patients enrolled in this study.
| Case | Positioning time(min) | Fluoroscopy shots | Positioning error(mm) | Harris Hip Score | Visual Analogue Scale | ||
| Before | After | Before | After | ||||
| 1 | 13 | 6 | 2.83 | 82 | 89 | 6 | 4 |
| 2 | 9 | 6 | 0.35 | 86 | 85 | 4 | 3 |
| 3 | 9 | 4 | 2.05 | 88 | 89 | 5 | 3 |
| 4 | 10 | 5 | -5.01 | 73 | 85 | 7 | 4 |
| 5 | 8 | 6 | -1.52 | L:84 | L:88 | L:4 | L:3 |
| 6 | 14 | 4 | -4.13 | R:68 | R:82 | R:6 | R:4 |
| 7 | 11 | 7 | 3.97 | 74 | 84 | 7 | 4 |
| 8 | 10 | 5 | 3.55 | 81 | 89 | 5 | 3 |
| 9 | 9 | 8 | 19.73 | 74 | 82 | 6 | 4 |
| 10 | 8 | 4 | -5.76 | 62 | 81 | 8 | 5 |
Table 2: Surgical indicators and scores. The positioning time, fluoroscopy time, and puncture accuracy were calculated and are shown. The pre- and post-operative VAS score and Harris score are also shown in this table.
