Clinical data were retrospectively collected on 58 consecutive patients undergoing non-intubated video-assisted thoracoscopic surgery from January 2016 to December 2022. The patients were given a preoperative visit by the anesthesiologist and provided with a detailed explanation of the contents of the anesthesia informed consent form prior to the anesthesia. The patients were allowed to choose one of the two groups (the NIVATS group or GA group) of anesthesia, and they signed an informed consent form.
The patients in the GA group were induced with 0.04 mg/kg of midazolam, 2.5 mg/kg of propofol, 0.3 mg/kg of etomidate, 0.5 µg/kg of sufentanil, and 1.2 mg/kg of rocuronium. After the inotropic drugs had taken full effect, a visual laryngoscope was used to guide the transoral insertion of a double-lumen bronchial tube or a single-lumen tracheal tube with a bronchial occluder. Preoperative radiography of the chest was performed, and the tracheal internal diameter was measured at the level of the sternoclavicular joint. A 41 Fr was selected if the tracheal internal diameter was ≥19 mm, a 39 Fr was selected for a tracheal inner diameter of ≥17 mm, a 37 Fr was selected for a tracheal inner diameter of ≥15 mm, a 35 Fr was selected for a tracheal inner diameter of ≥13 mm, and a 32 Fr was selected for a tracheal inner diameter of ≥11 mm. After the insertion of the double-lumen tube, the position of the tube was assessed and adjusted with a fibreoptic bronchoscope in the horizontal and lateral positions. Intraoperative anesthesia was maintained with a continuous infusion of 2-6 mg/kg/h of propofol and 0.25 µg/kg/min of remifentanil, all of which were delivered as intravenous anesthesia. The surgeons and patients undergoing non-intubated video-assisted thoracoscopic surgery are seen in Figure 1, Figure 2, and Figure 3.
Two research assistants (G.B. and L.W.J.) collected perioperative information from the patients, including on their age, BMI, anesthesia, duration of surgery, intraoperative bleeding, length of stay in the hospital, length of stay in the ICU, medical history, post-operative chest radiograph results, and their temperature and other laboratory tests performed on each post-operative day until discharge.
Measures of post-operative pulmonary complications (PPCs)
Referring to the guidelines published by the European Joint taskforce for perioperative clinical outcome (EPCO) definitions and taking into account the characteristics of this study18, the PPCs diagnostic tool was as follows: (i) pneumothorax: air inside the pleural space; (ii) pleural effusion: a chest radiograph with blunting of the costophrenic angle and loss of the sharp silhouette of the same side of the upright hemidiaphragm; (iii) pneumonia: use of new antibiotics, radiographic changes, fever, or a white cell count >12,000 µL−1; (iv) atelectasis: pulmonary opacification with mediastinum, hilum, or hemidiaphragm shifting toward the affected area; (v) pulmonary embolism: not defined; and (vi) acute respiratory distress syndrome (ARDS): PaO2:FIO2 ≤ 300 in the ventilated state and bilateral infiltrates on the chest radiograph.
Statistical analysis
For data analysis, 95% confidence intervals were used. A value of P < 0.05 was considered statistically significant. The lost data was adjusted for by using two-way interpolation. Continuous variables were represented as the average (standard deviation [SD]) or medium number (quartid digits range), and an independent-samples t-test or Mann-Whitney U-test was used for comparison. Categorical variables were presented as numbers and were compared by a Pearson's chi-squared test, a Fisher's exact test, or a continuous-corrected chi-square test. The above data analysis was conducted and completed by two data analysts independently. All the statistical analyses were performed with the SPSS26.0 software.
Resultados
Overall, 58 patients were eligible for analysis, including 31 patients in the GA group and 27 patients in the NIVATS group. The clinical characteristics of the two groups are shown in Table 1. There were no significant differences between the two groups in terms of gender, age, BMI, and ASA scores (P > 0.05).
Primary outcomes
The pulmonary complication rate was significantly lower in the NIVATS group (3.7%; one patient) compared with the GA group (25.8%; eight patients) (P = 0.051). Firstly, six patients in the GA group developed post-operative pneumothorax; however, no patients in the NIVATS group developed pneumothorax. The difference between the two groups was statistically significant (P = 0.026). Secondly, three patients in the GA group developed pleural effusion compared to one patient in the NIVATS group, although the difference between the two groups was not statistically significant (P = 0.707). Moreover, seven patients in the GA group developed pneumonia compared to none in the NIVATS group, and the difference between the two groups was statistically significant (P = 0.012).
In addition, three patients in the GA group developed pulmonary atelectasis compared to none in the NIVATS group. In the GA group, two patients developed pulmonary embolisms compared to none in the NIVATS group. No significant differences were found between the two groups in terms of pulmonary atelectasis or pulmonary embolism (P = 0.240 and P = 0.494, respectively). In the two groups, no patients developed ARDS.
Secondary outcomes
The use of non-intubated thoracoscopic anesthesia significantly reduced the intraoperative blood loss (100 mL [50-200] vs. 20 mL [5-50]; P < 0.001). Additionally, the NIVATS group had a shorter mean surgery duration (P = 0.024) and PACU stay time (P = 0.004). Furthermore, the difference in the day when the chest drain was removed between the NIVATS group and the GA group was significant (day 3 [2-4] vs. day 2 [1-3], respectively; P < 0.001). Moreover, the difference in the amount of post-operative chest drainage between the NIVATS group (260 mL [100-380]) and the GA group (672 mL [452.5-1,197.5]) was significant (P = 0.001). In the GA group, there were three patients who had a prolonged stay (>48 h) in the ICU, compared to no patients in the NIVATS group (P = 0.240). In the GA group, four patients had post-operative chest tightness and shortness of breath compared to one patient in the NIVATS group (P = 0.483). Finally, compared with the GA group, the NIVATS group had significantly shorter hospital stay lengths (6 days [5-7] vs. 5 days [4-6]; P < 0.001).

Figure 1: The surgeon performing non-intubated video-assisted thoracoscopic surgery. Please click here to view a larger version of this figure.
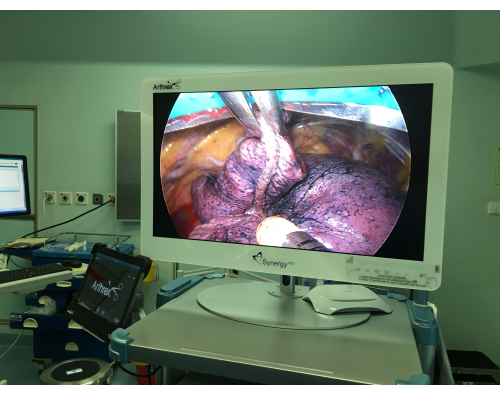
Figure 2: The affected lung under non-intubated video-assisted thoracoscopic surgery. Please click here to view a larger version of this figure.

Figure 3: A patient with a facial mask undergoing non-intubated video-assisted thoracoscopic surgery. Please click here to view a larger version of this figure.
Table 1: Patient demographics and post-operative results in each group. Please click here to download this Table.
