1. Preparation of equipment
- Wipe down the stereotaxic frame and pump with 75% ethanol to minimize bacterial contamination.
- Sterilize Hamilton syringe and fused silica needle.
Note: If chemical sterilization is used, be sure to rinse several times in sterile water before use. - Wipe surface of paraffin wax paper with 75% ethanol and allow to dry.
2. Preparation of mouse for injection
Note: Have mice delivered to your animal facility at least 7 days before the surgery to allow them to acclimate to the new environment and reduce stress.
- Weigh mouse for pre-operative baseline.
- Induce anesthesia with 30% Oxygen, 70% Nitrous oxide, and 4% Isoflurane until unresponsive to tail pinch
- Inject mouse with buprenorphine 0.1mg/kg intraperitoneally for post-operative analgesia
- Shave scalp
- Coat eyes with sterile petroleum jelly
- Prepare scalp with betadine x 3 wipes, then allow scalp to dry
- Make 1 cm midline sagittal incision of scalp using sterile surgical scalpel
Note: A generous incision will allow complete exposure of skull landmarks. - Shave 1 cm of ventral surface of tail beginning 1 cm from base and prepare with betadine x 3 wipes
- Place mouse on stereotaxic frame
Note: It is important to ensure mouse is secure in the frame with surface of skull parallel with the base of the frame, with excellent exposure of bregma and at least 3 mm to the right of bregma.
3. Intracerebral hemorrhage surgery
Notes: During the entire surgery the mouse is anesthetized with 30% Oxygen, 70% Nitrous oxide, and 1-3% Isoflurane, continuously maintained at 37 ± 0.5°C using a thermistor-controlled heating pad and monitored by rectal thermometer.
- Attach sterile 27 g needle on 1 cc syringe on frame.
- Adjust stereotaxic arm until needle is exactly over bregma.
- Adjust arm so that needle is at +2.5 mm lateral to bregma and lower to surface of skull.
- Manually rotate syringe to make burr hole on surface of skull while applying gentle downward movement of frame- taking care not to completely perforate skull.
- Remove needle and complete burr hole manually with syringe/needle
Note: Completing the burr hole by hand allows for immediate recognition when you have perforated the inner table of skull and minimizes risk of inadvertently pushing needle into brain parenchyma. - Make transverse incision on ventral surface of tail using sterile surgical blade and allow 2-3 large drops of arterial blood to fall onto paraffin wax paper. Then quickly stop bleeding with pressure using sterile gauze.
- Withdraw 17 μL blood into Hamilton syringe and place syringe on pump.
- Adjust stereotaxic arm to point 5° medially relative to vertical axis.
- Carefully adjust stereotaxic arm so that tip of the needle is over the burr hole in skull and then lower needle 3.5 mm.
- Wait 2 minutes then withdraw the needle 0.5 mm (so that tip is 3 mm deep)
- Wait 5 minutes to allow the brain to re-expand around the needle and minimize risk of blood refluxing up the needle insertion track during injection.
- Inject blood 1 μL/minute for 7.5 μL.
- Wait 5 minutes to allow initial blood clotting and for tissue shifts to occur to minimize elevations in intracranial pressure.
- Inject the remaining 7.5 μL at 1 μL/minute
- Allow needle to remain in place for 25 minutes to allow for blood clotting
Note: Failure to wait for blood clotting will result in blood refluxing up the needle insertion site when withdrawing the needle - Slowly withdraw the needle and immediately rinse with hot water to prevent any residual blood in the needle from clotting and ensure reusability of needle.
- Remove the mouse from the frame and close the tail and scalp incisions with veterinary surgical glue.
- Turn off anesthesia.
- Allow to mouse to awaken while being continuously warmed with free access to moistened food.
- Return mouse to cage with littermates when fully awake. Place wet food pellet on the bottom of cage to help animals in access to food.
4. Representative results:
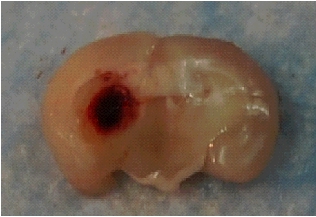
Figure 1. Coronal section of mouse brain 15 minutes after ICH surgery. Immediately after sacrifice the brain was inspected for ICH success based on gross inspection of a coronal section at the needle insertion site. Hemorrhages that tracked down to the base of the brain, up the needle track past the corpus callosum, or into the ventricles were deemed unsuccessful and that mouse was eliminated from all analyses. Overall ICH success rates were 75-85% in 50 mice with 0% mortality.
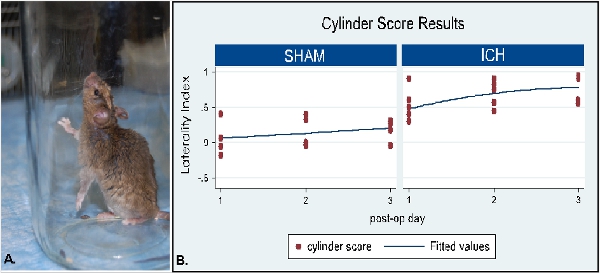
Figure 2. Cylinder testing demonstrates left hemiparesis after right basal ganglia ICH. (A) Sample mouse rear after ICH surgery. Note the placement of only the right forelimb on the wall of the cylinder after left basal ganglia ICH. (B) Graph of cylinder testing 1 results from cohort of mice after ICH surgery (n=5) compared to sham (n=4). Sham mice had all procedures except blood injection (needle was inserted into brain). Each mouse was placed in a 12-cm diameter clear glass cylinder and observed for 20 rears. The initial placement of the forelimbs on the wall of the cylinder was scored per rear. Subsequent movements (such as lateral exploration) were not scored until the mouse returned to the ground and the next rear scored. The laterality index was calculated as (# right forelimb placements on the side of the cylinder – # left forelimb placements)/(# right + # left + # both), where 0 indicated no forelimb preference and 1 indicated only the right forelimb was used.
