Twenty-four SLA-defined swine heterotopic hind limb transplants were performed using our modified technique with a mean ischemia time of 78 min (Range: 62-94 min). Graft inset and dorsolateral skin paddle positioning were achieved without difficulty in all animals. Near infrared laser angiography showed excellent graft perfusion in all recipients. The initial twelve venous anastomoses were performed using conventional suture techniques while the last twelve venous anastomoses were performed using a vascular coupling device. One animal with the conventional suture technique required a reanastomosis when a venous thrombus was identified immediately post-procedure. No complications were observed in any anastomoses performed with the coupling device. Recipient animals received a short course (30 days) of tacrolimus monotherapy with or without donor bone marrow (BM) infusion and co-stimulatory blockade. Tacrolimus dosing was adjusted to achieve target levels of 10-15 ng/ml. The short course tacrolimus only and untreated animals served as controls. The co-stimulation blockade based immunomodulatory protocol resulted in over 6 month survival post-transplant. There was no evidence of GVHD in any recipient. All long-term survivors (beyond 150 days post-transplant) had viable vascularized bone marrow at the time of euthanasia which demonstrates reliability of this model for investigating unique immunologic features of the bone marrow component of VCA (Figure 7).
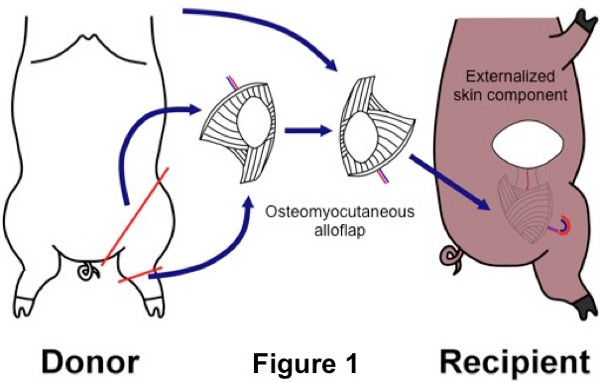
Figure 1. Schematic diagram of a swine heterotopic hind limb transplant. An osteomyocutaneous flap is harvested from the donor hind limb and transplanted to a subcutaneous pocket along the abdominal wall of the recipient.
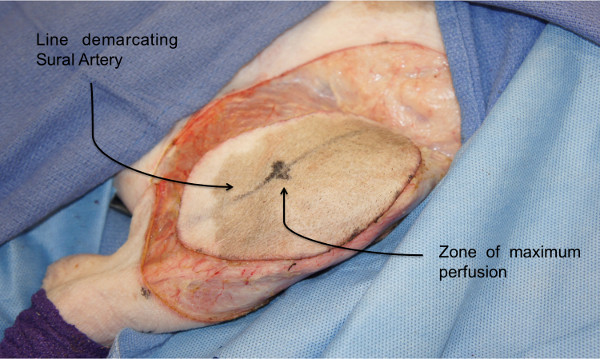
Figure 2: Osteomyocutaneous flap harvest: Donor skin paddle. Perforator zones in the anterolateral thigh are identified using laser angiography to demarcate the skin paddle of the osteomyocutaneous flap.
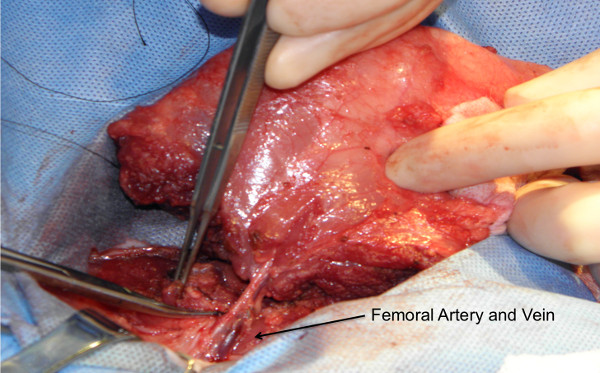
Figure 3: Osteomyocutaneous flap harvest: Graft on its vascular pedicle. Flap consisting of the distal femur, knee joint, proximal tibia, fibula, thigh muscles and skin paddle is harvested on a femoral vascular pedicle.
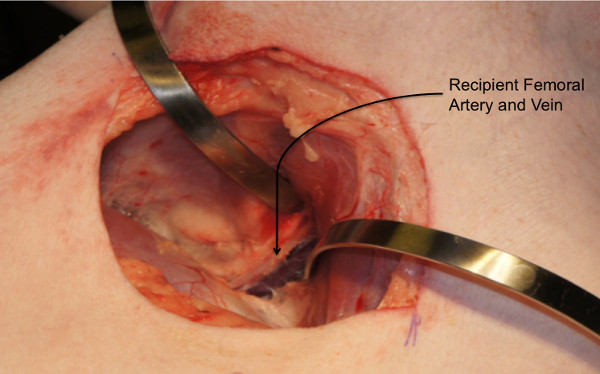
Figure 4: Recipient procedure: Creation of a subcutaneous abdominal pocket. Subcutaneous dissection is carried out to create an abdominal wall pocket extending from the groin to the dorsolateral abdominal wall.
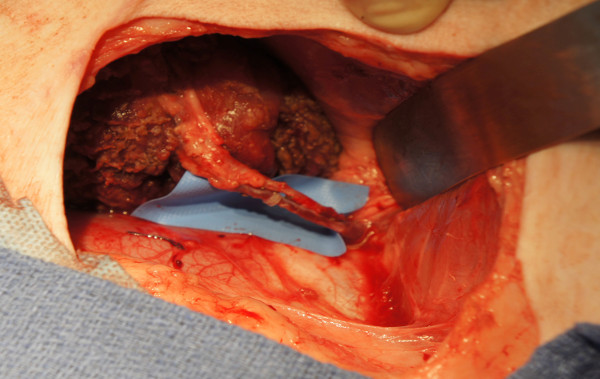
Figure 5: Recipient procedure: Graft inset and reperfusion following microvascular anastomosis. End-to-end femoral vessel anastomosis is performed after flap inset. The donor limb is used for the contralateral side of the recipient (i.e. the left donor limb for the right side of the recipient and the right donor limb for the left side of the recipient).

Figure 6: Skin component exteriorized to dorsolateral position for immune monitoring. During inset, the flap is positioned in a way that the skin paddle faces the dorsolateral abdominal wall where it is sutured to the recipient skin. This position allows easy monitoring of the flap.

Figure 7: Representative images from transplanted animals: (A) Long term survivor (>150 days) with no clinical evidence of rejection. (B) Long term survivor (>150 days) with no clinical evidence of rejection. The allograft was obtained from a donor with dark color skin. Both (A) and (B) received co-stimulation blockade (CTLA4Ig) based immunomodulatory therapy. (C) Negative control (short-term tacrolimus therapy only) with de-epithelialization and advanced rejection as soon as tacrolimus was withdrawn (Day 30).
