Here, we describe the process for creating a heterologous model of endometriosis in which the architecture of lesions is preserved by implanting fluorescently labeled pieces of human endometrium into immunocompromised mice, thus allowing non-invasive monitoring of lesion progression. Labeling of endometrial fragments is achieved by infection with adenovirus engineered to express mCherry, a protein emitting fluorescence in the near infrared region. In Figure 1, we show representative images of human endometrial fragments infected with Ad-mCherry observed under the fluorescence microscope. For illustrative purposes, both labeled and non-labeled fragments are included so differences in fluorescence between infected and non-infected tissues (autofluorescence) can be noted. During monitoring, in addition to the reference wavelength for mCherry, fluorescent images are taken with different pairs of excitation/emission wavelengths filters (Figure 2) to define the characteristic fluorescent emission profile of tissues. The purpose of this action is to "unmix" actual fluorescence emitted by lesions from background and autofluorescence emitted by host tissues and scar originated during surgery respectively. An illustrative example of the unmix process is shown in Figure 3. Estimations of variation in lesion size is performed by quantifying and normalizing fluorescent signaling emitted by lesions during the time course. For this purpose, images of monitoring containing raw fluorescence emitted by animals during each time point are first brought together unnormalized (Figure 4) in a single file. Subsequently fluorescence is unmixed, normalized and represented as a false color image (Figure 5). Finally, ROIs corresponding to specific lesion and background signaling are automatically recognized by the program and quantified (Figure 6). Background ROI signaling is subtracted from lesion ROI signaling and results of intensity in each time point are normalized against the time point at which intensity is maximal (Figure 7). At the end of the monitoring process, several weeks after surgery mice are sacrificed and viable implant can be recovered attached to the mouse peritoneum (Figure 8).
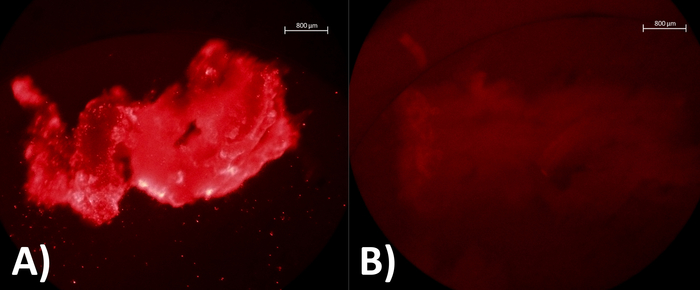
Figure 1: Visualization of endometrial fragments with fluorescence microscope after Ad-mCherry infection. (A) Human endometrial fragment incubated with Ad-mCherry at 37 °C and 5% CO2 during 24 h as a positive sample. (B) Human endometrial fragment incubated at 37 °C and 5% CO2 without Ad-mCherry as a negative control sample. Please click here to view a larger version of this figure.
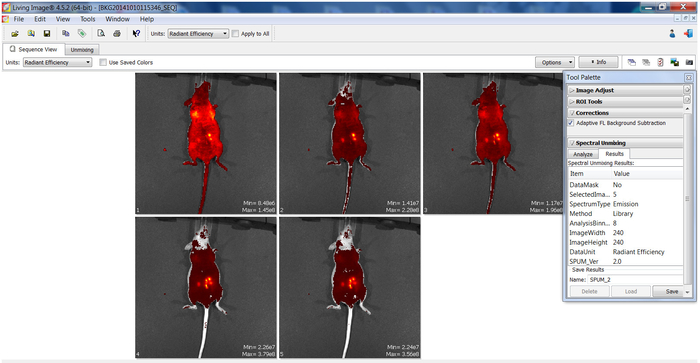
Figure 2: Raw imaging fluorescence emitted by labeled fragments implanted in mice. Picture shows representative imaging of raw fluorescence signal emitted by the same animal at a specific time point. Images correspond to screenshots obtained using software coupled to an in vivo imaging system device during a monitoring session. Each panel containing mice (numbered 1–5 in the left corner) corresponds to the fluorescence observed by using a different specific excitation/emission pair filter for acquiring images. Panel on the right (tool palette) show fluorescence parameters selected for acquisition of images Please click here to view a larger version of this figure.
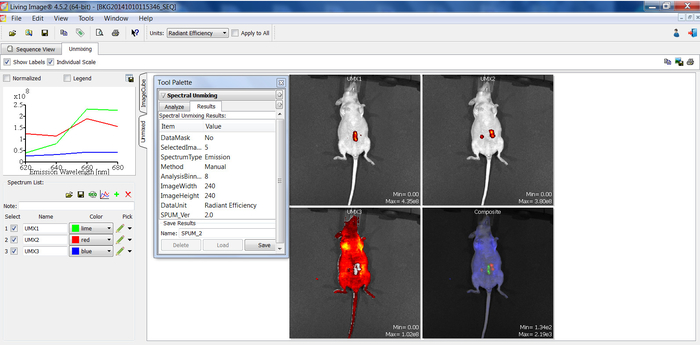
Figure 3: Unmixing of background vs specific fluorescence emitted by lesions. Picture shows representative images of the unmixing process performed to dissect actual fluorescence from lesions using the in vivo imaging system coupled software. Graph on the left panel denote normalized specific profiles of fluorescence emission by scar (green line, UMX1), lesions (red line, UMX2) and host tissue (blue line, UMX3 panel). Fluorescence intensity at different emission wavelengths (X-axis) is represented in units of radiant efficiency (Y-axis). Just note how each specific structure (i.e., scar, labeled lesions and host tissue) emits a different fluorescence profile which allows identifying and segregating them specifically form each other. On the right panel, fluorescence arising from launching specific emission profiles for scar (UMX1), lesions (UMX2) and host tissue (UMX3) are shown superposed on photograph images of mice. A composite image (Composite) is also included for illustrative purposes to denote the segmentation of fluorescence emitted by lesions from that emitted by scar or host tissues. Middle panel shows parameters selected for unmixing with the image software coupled to the in vivo imaging device Please click here to view a larger version of this figure.
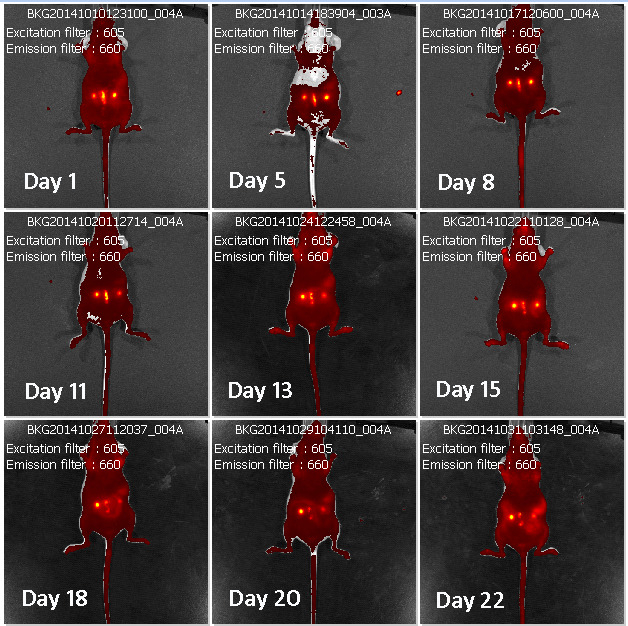
Figure 4: Time course monitoring of raw fluorescence emitted by lesions. Panel shows representative images of raw fluorescence emitted by a single mouse implanted with labeled human lesions (brilliant yellow spots) during the time course. Time points after surgery at which monitoring was performed are denoted as "Day (number)". Emission ad excitation pair filters used for monitoring are indicated in each panel/image. Each panel is identified by a specific code (BKG) in the upper part containing info related to the date at which fluorescence was acquired.
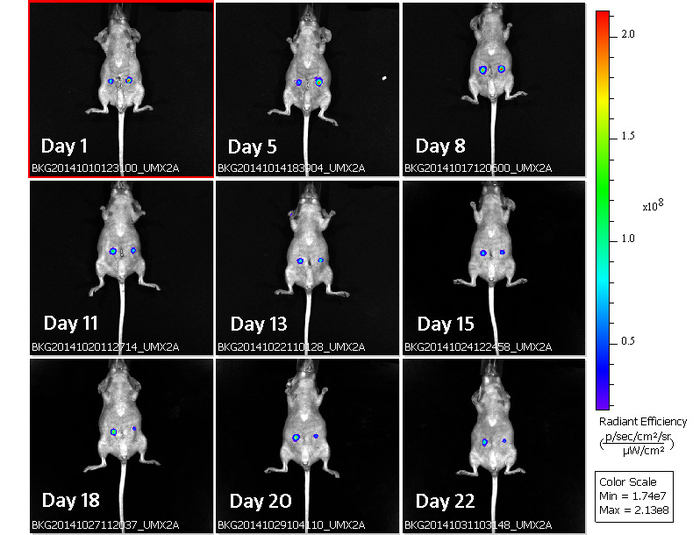
Figure 5: Time course monitoring of normalized fluorescence emitted by lesions. Representative images corresponding to unmixed, normalized fluorescent signaling emitted by human lesions (spots with rainbow color) superposed in a single mouse during the time course (days after surgery). Time points after surgery at which monitoring was performed are denoted as "Day (number)".Each panel is identified by a specific code (BKG) in the lower part containing info related to the date at which fluorescence was acquired. Rainbow palette color on the right side identifies fluorescence intensity (Radiant efficiency) emitted by lesions at each time point. Note how strong fluorescence intensity during the initial time points (i.e., red color in the center of lesions on days 1,5 and 8) declines during the time course (i.e., blue color in lesions on days 20 and 25). Please click here to view a larger version of this figure.
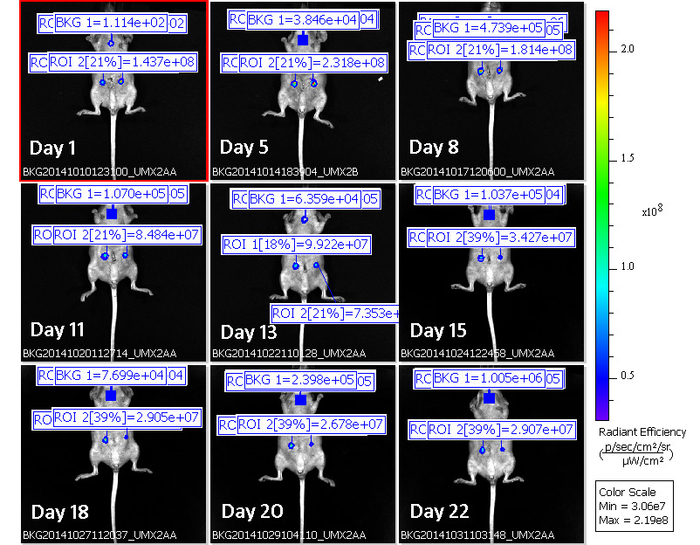
Figure 6: Use of ROIs for quantification of fluorescence intensity in lesions during the time course. Figure shows panel of images of normalized fluorescence emitted by lesions in a single mouse during the time course (i.e., Figure 5) with the addition of ROIs (delineating lesions and background) for quantification of fluorescence intensity. ROI 1 and ROI 2 identify the amount of fluorescence emitted by each of the two lesions during the time course. BKG identify the amount of fluorescence emitted by the host tissue (background fluorescence) during the time course. Background fluorescence is subtracted from ROIs for quantification purposes. Time points after surgery at which monitoring was performed are denoted as "Day (number)". Images acquired at each time point are labeled with a specific code (BKG) at the bottom of each one containing info related to the date at which fluorescence was acquired (first eight digits following BKG detail data for year(2014)-month (10) and -day(10 to 31)), an individual identification code (last 6 digits) and the specific profiles of fluorescence emission used for unmixing (UMX2) Rainbow palette color on the right side provides a visual scale of fluorescence intensity (Radiant efficiency) emitted by lesions at each time point. Note how fluorescence intensity values in the two lesions (ROI1 and ROI2) are higher at the initial time points (days 1 and 5) and decays during the time course to reach the lowest values at the end time points (days 20 and 25). Please click here to view a larger version of this figure.
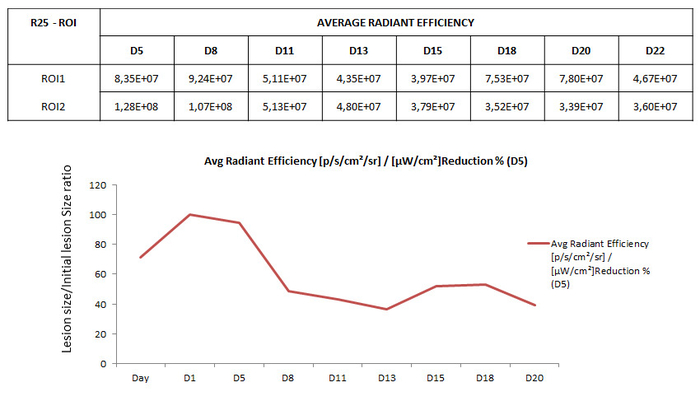
Figure 7: Normalization of fluorescence intensity during the time course. Table in the upper part shows illustrative example of the values of fluorescence intensity (radiant efficiency) emitted by two mCherry labeled lesions (ROI1 and ROI2) implanted in a mouse (R25). Monitoring of fluorescence was performed at different days after surgery (D5-D25) during the time course. D5- Graph at the bottom illustrates typical pattern of normalized fluorescence emitted by lesions infected with mCherry decaying during the time course. Y-axis shows values of fluorescence normalized to express the percentage of decay by using the formula (Signal intensity at each time point / Maximal signal intensity observed during the time course) x 100. Time points (Days (Dx) after implanting surgery) at which fluorescence was monitored are indicated in the X-axis. Note initial increase of signaling during the first 24 h after surgery, corresponding to stabilization of lesion, the peak in fluorescence intensity around D1-D5 and its subsequent decay due to episomal expression of mCherry during the time course Please click here to view a larger version of this figure.
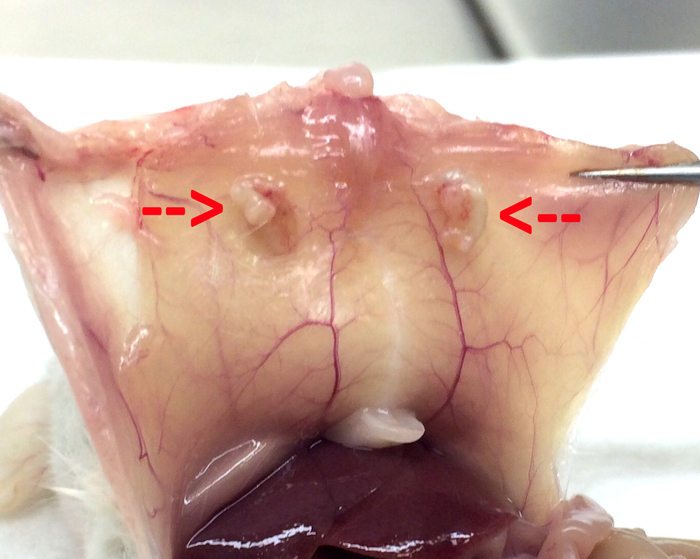
Figure 8: Macroscopic appearance of implanted endometriotic lesions. Representative images showing macroscopic appearance of endometriotic lesions implanted in mice at the end of the monitoring process upon sacrifice Please click here to view a larger version of this figure.
