A formal dedicated space for virtual broadcasts is not absolutely required and is limited by close access to the imaging technology. Figure 1 shows a makeshift broadcast studio with all the equipment described in this protocol (Figure 1A–D). The main setup is located in a room that houses the anatomy visualization table (Figure 1C) and includes the ultrasound laptop device (Figure 1A), and the adjacent hallway is used for setting up the anatomical specimen station to allow for the assembly of the overhead camera rig (Figure 1B).
Figure 2 includes sample video frame sequences from one of the heart-focused, virtual outreach sessions to demonstrate the types of screen formatting used to make the presentation visually appealing and enhance learning. Introductory information (e.g., a welcome slide, grant support, staff introductions, a brief session outline) is shown in a slide with a live presenter inset positioned off to the side (e.g., Figure 2A,I). This allows the presentation to be distinguished from regular slide presentations but maintains the video platform software feature of seeing the speaker.
Anatomical specimen demonstrations use a small presenter inset in the upper-left corner and the overhead camera as the main screen (Figure 2B). This allows the presenter to talk directly to the audience while demonstrating specific structures in a close-up view. Key point summary slides are shown as a simple slide alone, which enables the staff to move seamlessly behind the scenes from one station to another (Figure 2C,F,H) and helps students solidify main take-home messages. The strategically positioned monitors allow the staff to read the summary slide during the transition. The initial ultrasound view includes only a wide-angle view so that the presenter can introduce the SP, demonstrate the ultrasound laptop configuration, and introduce ultrasound and how the US probes work (Figure 2D).
An inset showing a closeup of the SP is included on the live US scanning since that helps students integrate what they are seeing with where the probe is being placed (Figure 2E). This is crucial for US since slight movements of the probe on the SP (e.g., rotating, sliding, or angling the probe) will change the resulting image. An inset is also used when the anatomy visualization table is being demonstrated because seeing the table manipulation is key to orienting the students and understanding what is being shown on the 3D reconstructions (Figure 2G). This is extremely important when near-peer presenters (e.g., high school and college students) are used so that middle and high school students can imagine themselves one day being able to manipulate the technology.
Table 1 lists the video switcher software control key setting specifications used to generate the various frames shown in Figure 2. The table indicates the names of each user-defined soft button, which camera is activated for the main screen, which camera is used for the PIP view, and the size and position of the PIP inset. These settings are the ones generated in steps 2.5.1-2.5.8 listed in the protocol.
Table 2 lists the behind-the-scenes production notes that are used by the staff member managing the broadcast to know when to manually select the proper camera and advance the slides to get ready for the next shot. Although the video switcher enables smooth transitions between shots, someone still has to make some behind-the-scenes selections to make the broadcast appear seamless. In addition, even with the video switcher and the multiport HDMI switcher, the HDMI inputs from the ultrasound laptop HDMI input and the anatomy visualization table HDMI input need to be manually switched. This can be done while projecting a US summary slide.
If a second video switcher is available, the ultrasound and anatomy visualization table HDMI inputs can be plugged into the second video switcher and its output plugged into the HDMI port that is normally shared by the two devices on the main video switcher. In this instance, a simple button press on the second video switcher changes the input to the main video switcher without having to replace HDMI cables. The ease of this arrangement may not be worth the added cost if the budget is limited. Alternatively, a second multiport HDMI switcher could be used.
The composite images shown in Figure 3 provide examples of the use of near-peer presenters in heart- and brain-focused outreach sessions. The use of heart models and specimens (inset) is shown in Figure 3A. The use of human cadaveric brain specimens and models (inset) is shown in Figure 3B. Figure 3 shows a 3D reconstruction of a CT scan in a patient with an occluded right coronary artery (Figure 3C, red arrow) and a coronary artery bypass graft (Figure 3C, black arrow). The use of wireless EEG recording of brain activity in an SP is shown in Figure 3D, including the raw EEG recordings (right panel) and the software visualization of the EEG activity in the brain (left panel). The recruitment of near-peer STEM role models is something that needs to be considered when broadcasting to middle and high school students. Near-peer high school presenters belonging to the STEM outreach team in this study were used to host virtual outreach sessions for children of staff working at a US federal agency during their sponsored "Take Your Child to Work Day" (a 30 min session on the heart29 and a 60 min session on the brain30).
The three-station integrated approach that was used in the described outreach presentations provides variety to the sessions and maintains student attention while using a web-based virtual video learning platform. More importantly, all three imaging modalities listed in the protocol require setting the stage for the students by reviewing some of the basic anatomy of the respective region (i.e., heart or brain). Virtual presentations can be easily tailored to the specific age and interest of the target audience. The protocol outlined in this paper has been used to provide virtual technology-focused STEM outreach presentations for a variety of middle and high school audiences, as well as teachers, across the state. A sample listing of these sessions is provided in Table 3.
To evaluate the effectiveness of the virtual outreach presentations, teachers were asked for their perceptions of the value of the sessions. The nine teachers who responded represent classes that together totaled ~150 high school students. Teachers were emailed surveys and asked to evaluate eight statements about the virtual outreach sessions using a 5-point Likert scale (see Table 4). The data were collected and statistically analyzed. A one-sample t-test (two-tailed) was used to determine if the evaluation responses were significantly different than an expected neutral point of the scale (3, neither agree nor disagree) and to determine the significance (p-value) for each statement, including upper and lower 95% confidence intervals. The frequency of responses is included in Table 4.
The teacher evaluations indicated that these virtual sessions were a valuable use of class time (p < .05) and that students, in the opinion of the teachers, learned something about STEM or technology during the virtual sessions (p < .01). The teachers strongly agreed with the statement that they would recommend the virtual outreach sessions to other teachers (p < .001) and would invite the team to conduct another virtual outreach session (p < .05). Together, the data from these first six statements confirm that the approach seems to be promising to provide a positive learning environment for students, despite being virtual. The final two questions asked about the level of engagement by those students attending the session either in person or virtually.
The neutral teacher evaluation data (i.e., no significantly higher or lower response compared to the neutral point) indicated that the students in their classes were not fully engaged by the virtual outreach sessions. The absence of a significant increase in this category of questions was not unexpected since hands-on activities engage students more than any virtual activity. The perceived value of the sessions by the teachers coupled with the absence of a significant negative evaluation for student engagement supports the use of these types of virtual outreach sessions when in-person, hands-on sessions are not possible.
Table 5 lists examples of the comments provided by students in the video platform chat bar on what they learned during the virtual sessions on the heart or brain. The presenter typically asks the class to provide examples of five things that they learned in the session that they did not know prior to logging into the virtual session. These comments indicated that students were paying attention during the outreach and that they were learning relevant content and confirmed the overall positive teacher evaluations.
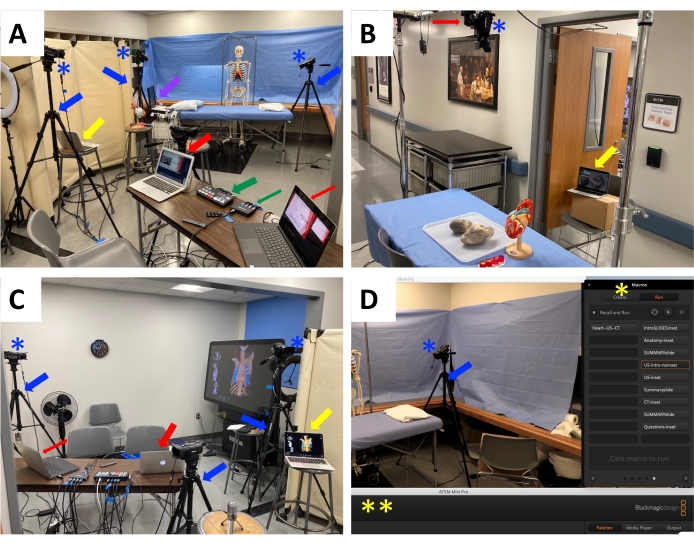
Figure 1: Makeshift broadcast studio with all the listed equipment. (A) View of the broadcast laptop (thick red arrow), slide presentation laptop (thin red arrow), video switcher (thick green arrow), HDMI multiport (thin green arrow), tripods (blue arrows) and mounted video cameras (blue asterisks), and ultrasound laptop (purple arrow). The camera near the broadcast laptop is aimed toward the hallway to capture the presenter at the anatomical specimen station. The tripod and camera on the left side of the photo provide the main camera view for the ultrasound station, while the cameras positioned at the head and foot of the massage table are used to provide close-up views of the SP during ultrasound scanning. The laptop denoted with the yellow arrow represents the broadcast monitor for the ultrasound station. (B) View of the anatomical specimen station with heart specimens and a heart model situated on the table and the overhead camera rig with its camera mount (red arrow) and video camera (blue asterisk) situated above the table. The laptop serving as the monitor for this station is denoted by the yellow arrow. (C) View of the CT imaging station with the vertically oriented anatomy visualization table (far-right side of image). The tripod (blue arrow) and video camera (blue asterisk) on the left of the image is the main camera view for the CT imaging station. The presenter at the anatomy visualization table station can simply watch the main broadcast laptop (thick red arrow) or the slide presentation laptop (thin red arrow) situated on the table. The laptop (yellow arrow) positioned on the stool on the right of the image is the monitor for the presenter at the ultrasound station. (D) Screenshot of the broadcast laptop during a live broadcast view of the ultrasound station with a tripod (blue arrow) and mounted video camera (blue asterisk) located at the foot of the massage table. The video switcher software control window (double yellow asterisks) is moved out of the way to the bottom of the screen. The macro popup window (single yellow asterisk with the macro buttons positioned to the right of the screen). Abbreviations: SP = standardized patient; CT = computed tomography. Please click here to view a larger version of this figure.
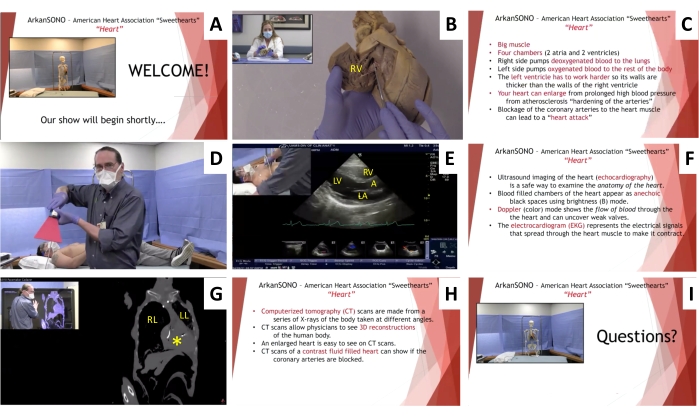
Figure 2: Sample video frames from a heart-focused virtual outreach session. (A) Example of introductory slides with live inset view from camera #1. (B) Anatomical specimen and model station with overhead camera view and live inset view from camera #2. The heart specimen has been opened to demonstrate the interior of the right ventricle. (C) Heart anatomy key point summary slide. (D) Ultrasound imaging station with live view from camera #3. (E) Ultrasound station with live inset view from camera #2 and ultrasound laptop video output. The scan is a parasternal long axis scan of the heart demonstrating the left atrium, left ventricle, right ventricle, and aorta. (F) Ultrasound imaging key point summary slide. (G) CT imaging station with live inset view from camera #4 and anatomy visualization table video output. The scan shows an enlarged heart (yellow asterisk) and the reduced size of the left lung compared to the right lung. (H) CT imaging key point summary slide. (I) Concluding questions from the audience slide with live inset view from camera #1. Abbreviation: CT = computed tomography; RV = right ventricle; LA = left atrium; LV = left ventricle; RV = right ventricle; A = aorta; LL = left lung; RL = right lung. Please click here to view a larger version of this figure.
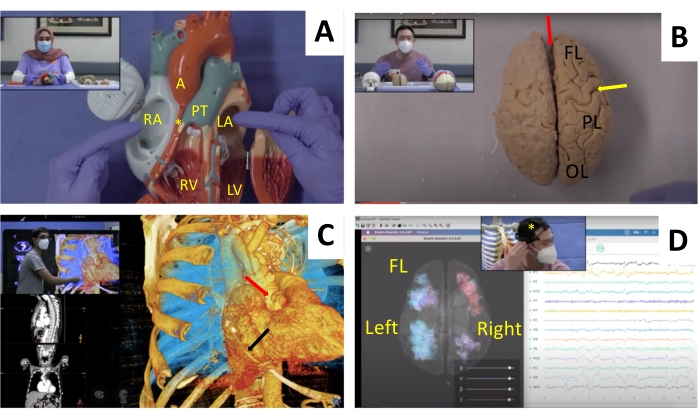
Figure 3: Using near-peer students in heart and brain presentations. Three near-peer students are shown as they present a virtual outreach session at the anatomy station (insets A,B) and anatomy visualization CT imaging station (inset C). One of these near-peer presenters served as the SP at the EEG station (inset D). Main images: (A) Heart model used to demonstrate the various parts of the heart, including the right atrium, pulmonary trunk, right ventricle, left atrium, left ventricle, and aorta. (B) Anatomical specimen station showing a whole human cadaveric preserved brain and the locations of the longitudinal fissure (red arrow), central sulcus (yellow arrow), frontal lobe, parietal lobe, and occipital lobe. (C) CT imaging using the anatomy visualization table showing an example of a heart scan with coronary artery bypass surgery with an occluded right coronary artery (red arrow) and the bypass graft vessel (black arrow). (D) Composite screen image showing EEG recording in an SP using a wireless EEG headset (yellow asterisk, inset panel), EEG recordings from the 14 leads of the headset (right panel), and brain visualization software reconstruction with a superior view of the brain localizing the EEG activity (left panel) in the left or right half of the brain. The frontal lobe is positioned at the top of the image. Abbreviations: CT = computed tomography; EEG = electroencephalogram; FL = frontal lobe; SP = standardized patient; RA = right atrium; PT = pulmonary trunk; RV = right ventricle; LA = left atrium; LV = left ventricle; A = aorta; FL = frontal lobe; PL = parietal lobe; OL = occipital lobe. Please click here to view a larger version of this figure.
| Macro Soft Panel Button # | Saved Macro Button Name | Key Settings on ATEM Mini Pro |
| 1 | IntroSlides-inset | Cam 4; On Air; Cam 2 DVE; X position=-7.3; Y position = 0.3; X size = 0.49; Y size = 0.49 |
| 2 | Anatomy-inset | Cam 1; On Air; Cam 2 DVE; X position = -10.2; Y position = 5; X size = 0.38; Y size = 0.38 |
| 3 | Anat-SummarySlide | Cam 4 |
| 4 | US-Intro-noinset | Cam 2 |
| 5 | US-inset | Cam 3; On Air; Cam 2 DVE; X position = -10.2; Y position = 5; X size = 0.38; Y size = 0.38 |
| 6 | US-SummarySlide | Cam 4 |
| 7 | CT-inset | Cam 3; On Air; Cam 2 DVE; X position = -10.2; Y position = 5; X size = 0.38; Y size = 0.38 |
| 8 | CT-SummarySlide | Cam 4 |
| 9 | Questions-inset | Cam 4; On Air; Cam 2 DVE; X position = -7.3; Y position = 0.3; X size = 0.49; Y size = 0.49s |
Table 1: Sample video switcher software control settings used for creating the heart video frames shown in Figure 2. The table lists the individual macro soft panel buttons, the corresponding button names, and the key settings on the virtual switcher software to enable various digital video effects. Abbreviations: CT = computed tomography; US = ultrasound; DVE = digital video effects.
| Shot Sequence # | Soft Button Panel Selection | Additional Action to Prepare for Next Shot |
| 1 | Begin with IntroSlides-inset | [Presenter advances slides with remote] |
| 2 | Switch to Anatomy-inset | press camera 2 on remote and advance slides |
| 3 | Switch to Anat-SummarySlide | press camera 1 on remote |
| 4 | Switch to US-Intro-noinset | advance slides |
| 5 | Switch to US-inset | press camera 3 on remote |
| 6 | Switch to US-SummarySlide | press camera 4 on remote then replace US with SECTRA HDMI cable on ATEM |
| 7 | Switch to CT-inset | advance slides |
| 8 | Switch to CT-SummarySlide | press camera 1 on remote |
| 9 | Switch to Questions-inset and advance slides |
Table 2: Sample broadcast shot record for the heart presentation. The table lists the shot sequence, soft panel button selection, and additional actions required to prepare for the next shot in the virtual broadcast. Abbreviations: CT = computed tomography; US = ultrasound.
| Group Description # | Student Grade | Virtual Outreach Topic | Stations |
| Middle school PreAP science class | 8 | Ultrasound and Infrared imaging | Measuring the speed of sound & infrared imaging |
| Summer Science STEM fair | 6th – 8th | Skeletal demonstration | Anatomical specimen station |
| Weekly Anatomy and Technology Interactive – Summer Program 2020, 2021 | 6th through 12th | Heart | Heart anatomy, US of heart, CT imaging of heart |
| Weekly Anatomy and Technology Interactive – Summer Program 2020, 2021 | 6th through 12th | Lung | Lung anatomy, US of respiratory system, CT imaging of respiratory system |
| Weekly Anatomy and Technology Interactive – Summer Program 2020, 2021 | 6th through 12th | Brain/CNS | Brain and spinal cord anatomy, US nerves, CT imaging of skull and brain. |
| Weekly Anatomy and Technology Interactive – Summer Program 2020, 2021 | 6th through 12th | US of regions throughout the body | Ultrasound station |
| Weekly Anatomy and Technology Interactive – Summer Program 2020, 2021 | 6th through 12th | CT imaging of regions throughout the body | SECTRA station |
| High school science class | 9th | Heart | Heart anatomy, US of heart, CT imaging of heart |
| High school science class | 9th | Brain | Brain anatomy, CT/MRI imaging of skull and brain, EEG recording of live SP |
| Student Athlete STEM Academy (SASA)- Summer Program | 9th – 12th | Muscle, tendons, joints, skeleton, heart, brain, skull | Model and skeleton demonstrations, US imaging of common sports injury sites, CT imaging of common MSK injuries, heart anatomy |
| Health Professions Recruitment and Exposure Program (HPREP) | 9th – 12th | Heart | Heart anatomy, US of heart, CT imaging of heart |
| Rural school district high school science classes | 9th-10th | Heart | Heart anatomy, US of heart, CT imaging of heart |
| Rural school district high school science classes | 9th-10th | Brain and CNS | Brain anatomy, CT imaging of skull and brain |
| American Heart Association “Sweethearts” Program | 10th | Heart | Heart anatomy, live US scanning of SP heart , EKG recording of heart pacemaker activity, CT imaging of heart |
| Cancer program – Summer (upper level high school and college) | 11th and 12th and college | Review of cancer types, histology and pathology | Anatomy of major organs affected by cancer, US and CT imaging of these organs, virtual histopathology of cancer in these organs |
| Arkansas Science Festival | open to all interested grades | heart | anatomy, US, CT |
Table 3: Virtual STEM outreach presentations and target audience. The table lists descriptions of representative student groups reached through outreach sessions, their grade levels, the main topic of the outreach, and the various stations included in the outreach. Abbreviations: CT = computed tomography; US = ultrasound; STEM = science, technology, engineering, and mathematics; CNS = central nervous system; EEG = electroencephalogram; MRI = magnetic resonance imaging; EKG = electrocardiogram. # Some student groups were recruited directly through known contacts, while others were recruited via website postings.
| One Sample t test (two-tailed) | ||||||||||
| Likert Response (Frequency)# | Average Evaluation | Standard Deviation | t | df | p-value | 95% CI (lower, upper) | ||||
| I believe this virtual classroom outreach visit was a valuable use of class time | 1(0), 2(2), 3(0), 4(0), 5(7) | 4.33 | 1.32 | 3.024 | 8 | .017 * | 3.316, 5.350 | |||
| The topic was presented at an appropriate level for my students | 1(0), 2(0), 3(0), 4(4), 5(5) | 4.56 | 0.53 | 8.854 | 8 | .000*** | 4.150, 4.961 | |||
| I would recommend this outreach session to other teachers | 1(0), 2(0), 3(2), 4(1), 5(6) | 4.44 | 0.88 | 4.913 | 8 | .001 ** | 3.767, 5.122 | |||
| I would welcome the ArkanSONO team to conduct virtual outreach sessions next year in my classes | 1(0), 2(2), 3(0), 4(0), 5(7) | 4.33 | 1.32 | 3.024 | 8 | .017 * | 3.316, 5.350 | |||
| I believe my students learned new STEM content in this session | 1(0), 2(0), 3(2), 4(2), 5(5) | 4.33 | 0.87 | 4.619 | 8 | .002 ** | 3.668, 4.999 | |||
| I believe my students learned something about technology in this session | 1(0), 2(0), 3(2), 4(2), 5(5) | 4.33 | 0.87 | 4.619 | 8 | .002 ** | 3.668, 4.999 | |||
| My in class students were engaged with this activity | 1(0), 2(4), 3(0), 4(3), 5(2) | 3.33 | 1.32 | 0.756 | 8 | .471 | 2.316, 4.350 | |||
| My online students were engaged with this activity | 1(2), 2(2), 3(1), 4(2), 5(2) | 3.00 | 1.58 | 0.000 | 8 | 1.00 | 1.784, 4.215 | |||
| # 5-point Likert scale | * p<.05 | |||||||||
| ** p<.01 | ||||||||||
| *** p<.001 | ||||||||||
Table 4: Teacher evaluation of the virtual outreach sessions. The table lists the teacher responses to eight different program evaluation questions using a 5-point Likert scale and the statistical analysis of the responses. Abbreviations: STEM = science, technology, engineering, and mathematics; df = degrees of freedom; CI = confidence interval.
| Heart Session Comments | I learned about the different chambers of the heart, also about ventricles, also I learned how an ultrasound works. | |||||
| I learned how to identify the pericardial sack with ultrasound and possibly what to expect with bleeding | ||||||
| I didn't know ultrasounds could be used on different parts of the body other than the abdominal cavity | ||||||
| I learned that the sound of your heart beating is the valves opening and closing | ||||||
| I didn't know how urine went through the bladder | ||||||
| Ultrasound uses sound waves to see structures of the body, I thought it was like an x-ray. | ||||||
| I learned what to look for and what things actually looked with an ultra-sound. | ||||||
| I didn't know that you could see how all the muscles are moving on the ultrasound | ||||||
| What bone looks like on an ultrasound and that an ultrasound uses sound waves. | ||||||
| Before this zoom I did not know the purpose for the gel | ||||||
| I knew that X-rays weren't safe, but I didn't know that ultrasounds are safe! | ||||||
| Brain Session Comments | I learned how different an Alzheimer patients brain looks than ours | |||||
| I did not know that stroke symptoms vary depending on what part of the brain is affected. | ||||||
| I didn't know that you could put an EEG on your head and see the brain activity! That was super cool! | ||||||
| I did not know that the frontal cortex did not fully develop until a person is in their late 20s | ||||||
| I didn't know we could see the brains activity with a headset, I think it is really cool to think about Alzheimer's make the gyri shrink | ||||||
| I didn't realize that babies skulls didn't fully fuse together until they grow up. | ||||||
| I learned about the effects of aneurisms | ||||||
| I learned the brain has two layers that protect it | ||||||
| Your brain can look different and have a bunch of grooves from certain diseases brains and some functions they have | ||||||
| I learned how the electrodes read the movement in the brain. | ||||||
| I learned that CT is a 3D modal to see more details | ||||||
| I learned that if you are right hand dominant then you use your left brain | ||||||
Table 5: Student comments-What did you learn today? The table provides representative student comments on what they learned in separately conducted brain and heart outreach sessions. The student comments were copied from the chat bar at the conclusion of the virtual outreach session.
