The inspection of cardiac function by "eyeballing" can be applied to qualitatively assess the global cardiac systolic function. Any suspicion of impaired cardiac function should lead to an urgent HC with pediatric cardiology for the assessment of congenital heart disease (CHD). Treatment must be started according to the pathophysiology, and the treatment should be integrated and modified according to a comprehensive anatomical and functional echocardiography study27. If ductal-dependent CDH is suspected, prostaglandins must be started, and a pediatric cardiology consult must be scheduled. In the study center, pediatric cardiology and neonatal hemodynamics consultation services are available.
From January 2019 to July 2022, a total of 1,045 HC/POCUS studies were carried out in our hospital, of which 25 corresponded to the protocol (2.3%). The type of decompensation was classified as respiratory in 14 newborns, hemodynamic in 8 newborns, and cardiac arrest-related (one PEA and one tamponade) in 3 newborns. The ultrasound protocol diagnoses were PTX (12), PE (4), PCE/CT (3), altered contractility (2), cardiac arrest-related (2), mobilization of the endotracheal tube (1), and hypoglycemia (1).
The protocol and interventions were performed by an expert neonatologist with advanced ultrasound training in 8 patients, by neonatology fellows supervised by an expert in 12 patients, and by fellows exclusively in 5 patients (including the resolution of three tension PTX cases and two tamponade drains). Most (96%) of the patients survived the event, and 68% survived to discharge. Overall, 19 procedures were performed (five chest tubes, three chest tube corrections, four pneumothorax needle drainages, four pleural effusion needle drainages, and three tamponade needle drainages), an endotracheal tube adjustment was performed, and one glucose bolus was administered. The chest X-ray (CXR) corresponding to each event was found in the electronic system at a median (interquartile range) of 58 (27-97) min. Table 3 details the institution's experience with this protocol.
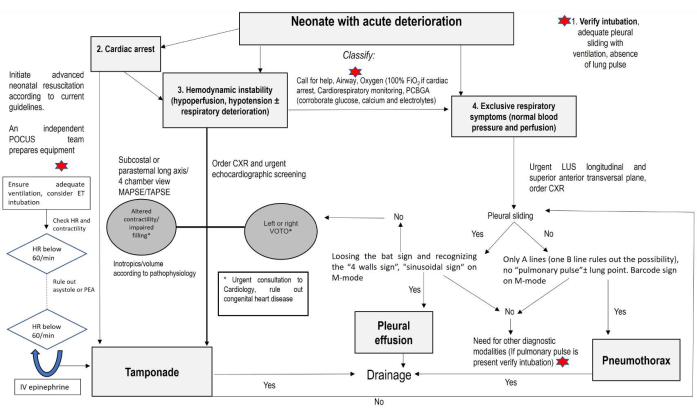
Figure 1: Algorithm: A modified sonographic algorithm for life-threatening emergencies in the critically ill newborn. Start by assessing the airway if the newborn is intubated, perform the consolidated core steps to ensure the newborn is monitored, and obtain the PCBGA. If the infant is in cardiac arrest, assistance (image acquisition) can be provided in two steps: a) performing corrective steps to detect the HR and effective cardiac output and ensure a real asystole; b) performing advanced CPR to rule out PCE/CT and hypovolemia and performing LUS to detect PTX. If hemodynamic instability (hypoperfusion, hypotension, with or without respiratory deterioration) is present, assess contractility, assess the left or right VOTO, and rule out PCE/CT. If negative or exclusive respiratory symptoms (normal blood pressure and perfusion) are present, rule out PTX and PE. Abbreviations: PCBGA = point of care blood gas analysis; POCUS = point of care ultrasound; ET = endotracheal; HR = heart rate; PEA = pulseless electrical activity; MAPSE = mitral annular systolic excursion; TAPSE = tricuspid annular systolic excursion; CXR = chest X-ray; VOTO = ventricular outflow tract obstruction; PCE/CT = pericardial effusion/cardiac tamponade; PTX = pneumothorax; PE = pleural effusion. Please click here to view a larger version of this figure.
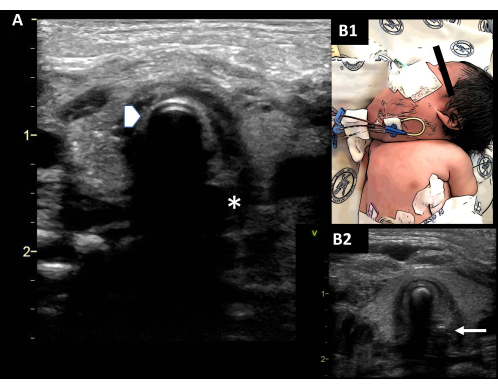
Figure 2: Verifying intubation. (A) Observe the outline of the ETT (double rail image, arrowhead), which generates a posterior shadow. The esophagus on the left of the screen is collapsed (asterisk). (B1) Difficult airway in a newborn with lymphangioma. (B2) The ETT is observed in situ; a small orogastric tube is observed (arrow). Abbreviation: ETT = endotracheal tube. Please click here to view a larger version of this figure.
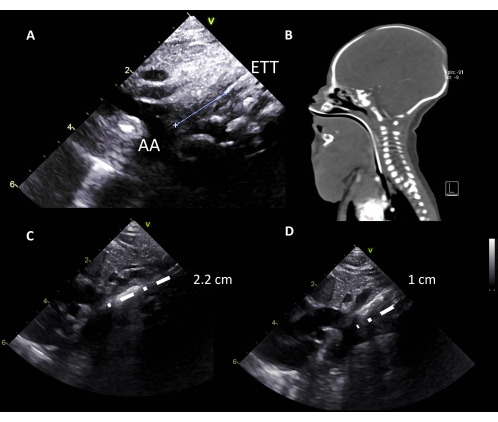
Figure 3: ETT depth. (A) The aortic arch is considered an orientation point to locate the carina, and the ETT is located at 1 cm from the AA. (B) Difficult airway in a newborn with lymphangioma; a high ETT is detected. (C) A high ETT (2.2 cm from the AA) is seen on the ultrasound and corrected. (D) Correctly placed ETT (1 cm from the AA). Abbreviations: AA = aortic arch; ETT = endotracheal tube. Please click here to view a larger version of this figure.
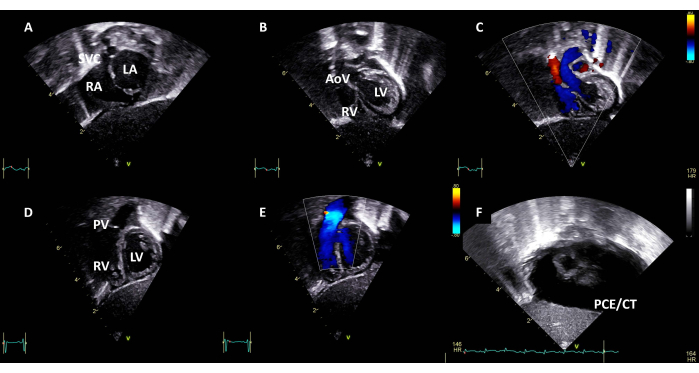
Figure 4: Subcostal long axis view. Sweeping from posterior to anterior, identify (A) the superior vena cava, the right and left atriums; (B) the right and left ventricles and the aortic valve; (C) color Doppler, indicating left ventricular outflow tract without obstruction; (D) and the crossing right ventricle and pulmonary valve. (E) Color doppler, indicating right ventricular outflow tract without obstruction. (F) Subcostal view with PCE/CT. Abbreviations: SVC = superior vena cava; RA = right atrium; LA = left atrium; RV = right ventricle; LV = left ventricle; AoV = aortic valve; PV = pulmonary valve; PCE/CT = pericardial effusion with cardiac tamponade. Please click here to view a larger version of this figure.
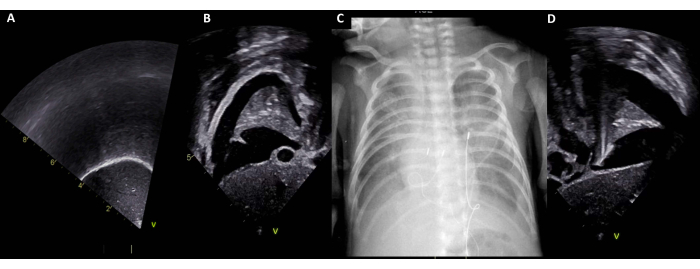
Figure 5: Transdiaphragmatic window. (A) Normal right transdiaphragmatic window. (B) Right PE. (C) Corresponding CXR with bilateral PE. (D) Left PE. Abbreviations: PE = pleural effusion; CXR = chest X-ray. Please click here to view a larger version of this figure.
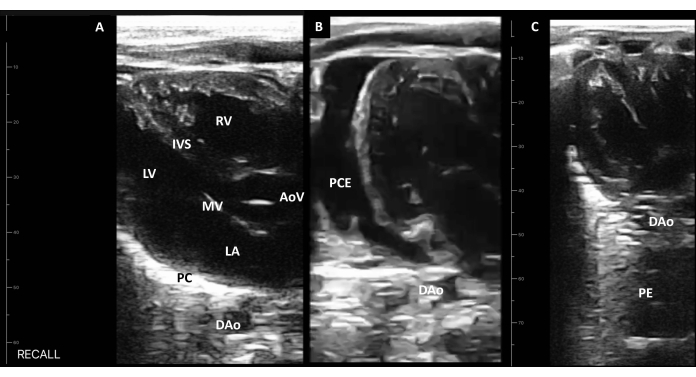
Figure 6: Handheld device long axis view. (A) Identify the right ventricle, the interventricular septum, the aortic valve, the left ventricle, the mitral valve, the left atrium, the pericardium, and the descending aorta. (B) The PCE identified as fluid anterior to the DAo. (C) The PE posterior to the DAo. Abbreviations: LA = left atrium; RV = right ventricle; LV = left ventricle; AoV = aortic valve; IVS = interventricular septum; MV = mitral valve; PC = pericardium; DAo = descending aorta; PCE = pericardial effusion; PE = pleural effusion. Please click here to view a larger version of this figure.
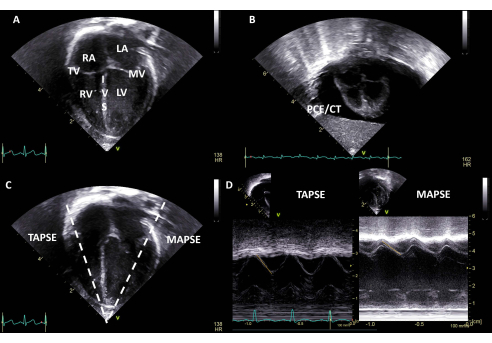
Figure 7: Four chamber view. (A) Identify the right atrium, the tricuspid valve, the right ventricle, the interventricular septum, the left atrium, the mitral valve, and the left ventricle. (B) Four chamber view with PCE/CT. (C) An M-mode image can be obtained on the tricuspid and mitral annulus to calculate the TAPSE/MAPSE. (D) TAPSE and MAPSE are depicted; the measurement in millimeters (mm) can be compared to gestational age nomograms. Abbreviations: SVC = superior vena cava; RA = right atrium; LA = left atrium; RV = right ventricle; LV = left ventricle; PCE/CT = pericardial effusion with cardiac tamponade; TV = tricuspid valve; MV = mitral valve; IVS = interventricular septum; TAPSE = tricuspid annular systolic excursion; MAPSE = mitral annular systolic excursion. Please click here to view a larger version of this figure.
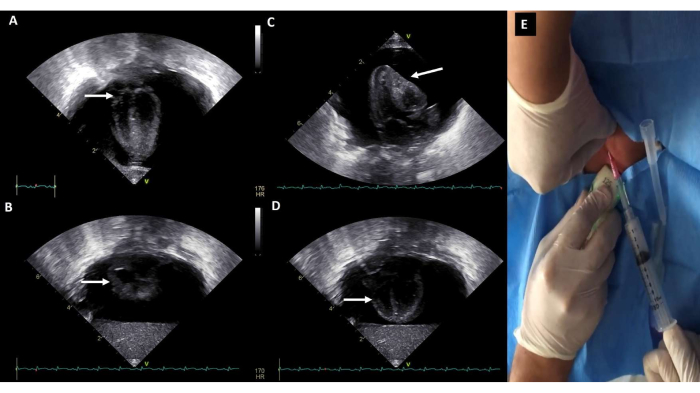
Figure 8: Pericardial effusion with cardiac tamponade. Large circumferential pericardial effusion. (A,B) A systolic right atrial collapse and (C,D) diastolic right ventricular collapse are observed qualitatively. (E) Pericardiocentesis. Please click here to view a larger version of this figure.
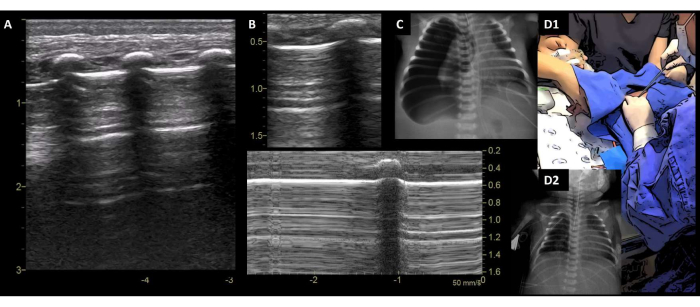
Figure 9: Pneumothorax. (A) PTX is diagnosed with absent pleural sliding, only A-lines, and no "lung pulse". (B) M-mode image shows the "Bar code sign". (C) Corresponding X-rays. (D1) Chest tube insertion. (D2) PTX resolved on a control CXR. Abbreviations: PTX = pneumothorax; CXR = chest X-ray. Please click here to view a larger version of this figure.
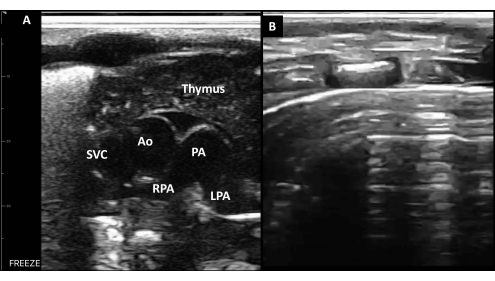
Figure 10: Anterior-superior transverse plane. (A) In a healthy newborn, the sternum and mediastinal structures, including the thymus, the superior vena cava, the aorta, and the pulmonary artery with its right and left branch, can be observed. (B) A-lines in the anterior transverse plane without sliding is a sensitive sign of anterior PTX. Abbreviations: SVC = superior vena cava; Ao = aorta; PA = pulmonary artery; RPA = right PA branch; LPA = left PA branch. Please click here to view a larger version of this figure.
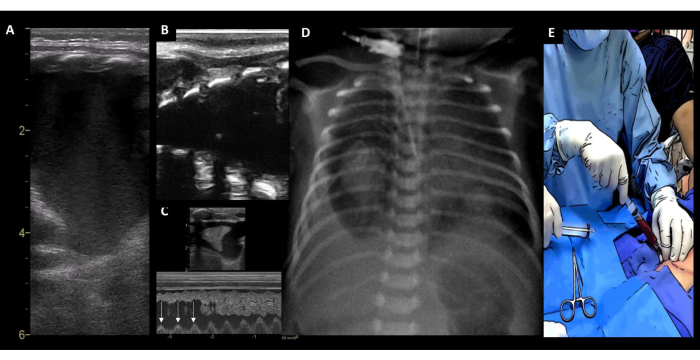
Figure 11: Pleural effusion. (A) PE identified by the absence of the bat sign and the "four walls sign" (high-end ultrasound equipment). (B) Same PE identified with a hand-held device. (C) M-mode image showing the "sinusoidal sign" (with each respiratory cycle, the lung surface line moves toward the pleural line, arrow). (D) Corresponding CXR. (E) Drainage of the hemothorax. Abbreviations: PE = pleural effusion; CXR = chest X-ray. Please click here to view a larger version of this figure.
Video 1: Lung pulse, deep ETT, and pneumothorax. A preterm newborn with respiratory decompensation and a suspected PTX, but a lung pulse was encountered; in verifying the ETT depth, a deep tube was recognized and retracted. The lung pulse disappeared, and a PTX was diagnosed. Parenchymal signs appeared after chest tube placement. The corresponding X-rays are shown. Please click here to download this Video.
Table 1: Ultrasound settings. Please click here to download this Table.
Table 2: Lung ultrasound semiology29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45. Abbreviations: PTX = pneumothorax; SVC = superior vena cava; PE = pleural effusion; ETT = endotracheal tube. Please click here to download this Table.
Table 3: Center experience. Abbreviations: DT = deterioration type; GA = gestational age; PDL = postnatal day of life; SF = supervised fellow; A = attending neonatologist; NF = neonatology fellow; SE = survived event; SD = survived discharge; Y = yes; N = no; RDS = respiratory distress syndrome; PDA = patent ductus arteriosus; VSD = ventricular septal defect; PO = post operated; ROP = retinopathy of prematurity; IVH = intraventricular hemorrhage; ETT = endotracheal tube; NEC = necrotizing enterocolitis. Please click here to download this Table.
