Short-term results of acetabular rim extension have previously been published, arising from an ongoing observational study at the Utrecht University Department of Clinical Sciences18. From December 2019 to March 2022, a total of 61 hips from 34 dogs were included in the study. The cohort consisted of 24 males and 10 females, with a median age of 12 months (ranging from 7 to 38 months) and a median body weight of 27.3 kg (ranging from 12 to 86 kg). Seven dogs underwent surgery on a unilateral hip, while twenty dogs underwent bilateral hip surgery in a single session. Additionally, seven dogs received surgery on both hips, conducted in two separate sessions.
The previous study found a significant increase in the Norberg Angle (NA), linear percentage of femoral head coverage (LFO), and percentage of femoral head coverage (PC) immediately after implantation (Table 1). Moreover, the postoperative Ortolani subluxation sign was negative in 96.7% of operated limbs indicating that the acetabular rim extension implant restored hip congruency and diminished laxity of dysplastic hips18. Particularly, the ability to increase coverage of the femoral head without performing any re-directional osteotomy allowed physiological pelvic geometry retainment. The minimally invasive technique resulted in low incidences of complications (4.9%) in the short-term, encouraged early mobilization, and decreased pain related to activity (Table 1).
Furthermore, this technique allowed single-stage bilateral 3DHIP implant placement. Treated limb(s) were weightbearing without pelvic support within 12 to 24 h after surgery. During the 12-month monitoring period, 3 dogs required revision surgery due to either implant failure (2 dogs) or a significant advancement of osteoarthritis (1 dog). Using the presented surgical approach simultaneously with the suggested hip joint movements (abduction, flexion, and external rotation), better exposure of the ventrocaudal aspect of the iliac shaft and craniodorsal aspect of the hip joint was obtained, facilitating 3DHIP implant positioning. In addition, intra-operative fluoroscopy increased the accuracy of implant positioning.
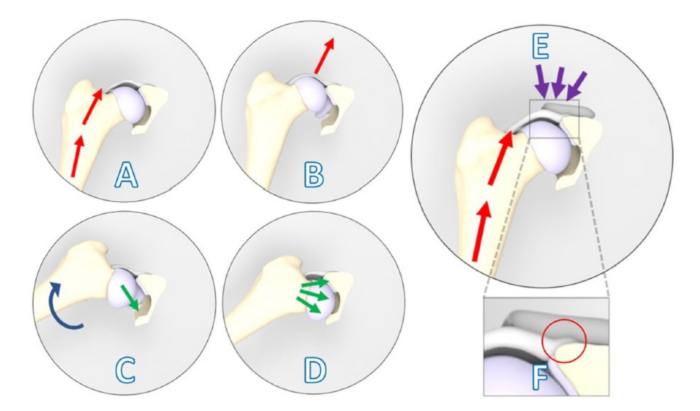
Figure 1: Schematic illustrations showing a positive Ortolani subluxation sign counteracted by the 3DHIP implant. (A–D) Positive Ortolani subluxation sign. (A) The dog's limb is positioned in neutral flexion and adduction, and a force (red arrows) is exerted towards the dorsum of the dog along the femoral axis that causes (B) dorsal subluxation of the dysplastic hip joint. (C) Gradual limb abduction (blue arrow) is performed while maintaining pressure on the femur. (D) Dependent on the acetabular rim deficiency, the subluxated femoral head falls back into the socket (green arrows). (E) The 3DHIP implant is introduced to enhance the stability of the dysplastic hip joint by reinforcing the hip capsule and labrum, which serve as weight-bearing and stabilizing surfaces (purple arrows). (F) Upon magnification of the rectangular area, the internal 1.5 mm offset of the implant is visible in the red circle, which ensures the capsule attachment remains unaffected. This figure was modified from Willemsen et al.17. Abbreviation: 3DHIP = 3-dimensional-printed, hip implant. Please click here to view a larger version of this figure.
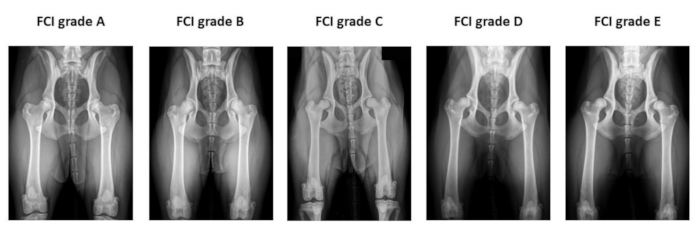
Figure 2: Example of the preoperative hip radiographs used for Fédération Cynologique Internationale hip dysplasia classification. Radiographs are taken in the ventro-dorsal hip extended position. From left to right, FCI classifies hip dysplasia into five different categories: A (normal), B (borderline), C (mild hip dysplasia), D (moderate hip dysplasia), and E (severe hip dysplasia). Abbreviation: FCI = Fédération Cynologique Internationale. Please click here to view a larger version of this figure.

Figure 3: Images of hip joint CT examinations illustrating osteophytes of varying sizes. The thickness of all featuring osteophytes is measured in both (A,B) coronal planes and (C) transverse planes at the cranial (white arrowhead) and caudal (red arrowhead) acetabular rim and femoral neck (black arrowhead). Dogs that have femoral neck and/or cranial and caudal acetabular rim osteophytes > 2 mm are excluded. CT examination slice thickness is 5 mm. Please click here to view a larger version of this figure.
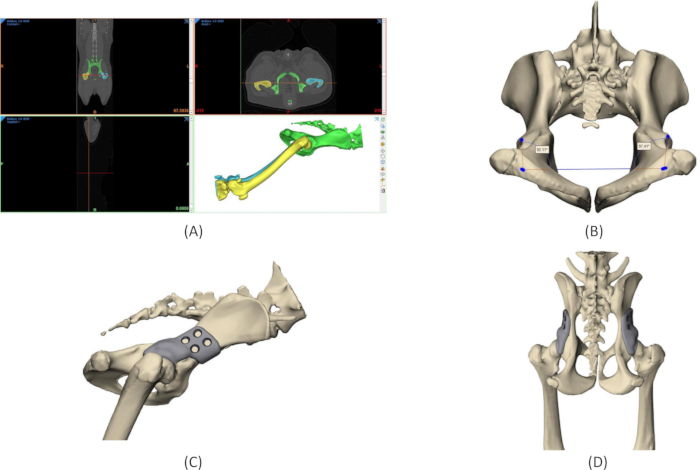
Figure 4: Design process of 3DHIP implant. (A) Segmentation of the region of interest from CT DICOM data. (B) Measurements of the native Norberg angles on the 3D model of the pelvis. (C) Rendering of a 3DHIP implant on the right hip, lateral view. (D) Rendering of bilateral 3DHIP implants, dorsal-ventral view. Abbreviation: 3DHIP = 3-dimensional-printed, hip implant. Please click here to view a larger version of this figure.
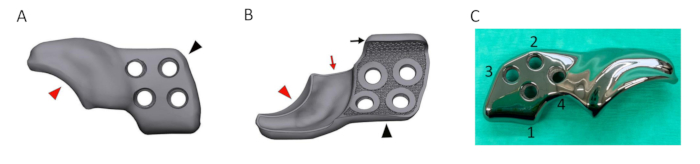
Figure 5: Rendering of a designed 3DHIP implant. (A) Rendered image of the lateral/outer side of the 3DHIP implant. (B) Rendered image of the inner implant surface showing the porous surface allowing bone ingrowth for osseointegration. The bone attachment part (black arrowhead) of rendered implant incorporating 4 locking screw holes and the ventral ilium flange (black arrow) for assisting in correct implant positioning and stabilization. The rim extension part (red arrowhead) of the rendered implant with the internal 1.5 mm offset (red arrow) allowing unhindered joint capsule attachment. (C) Photograph of a titanium 3DHIP implant showcasing 4 screw holes arranged in the sequence for screw insertion. Abbreviation: 3DHIP = 3-dimensional-printed, hip implant. Please click here to view a larger version of this figure.
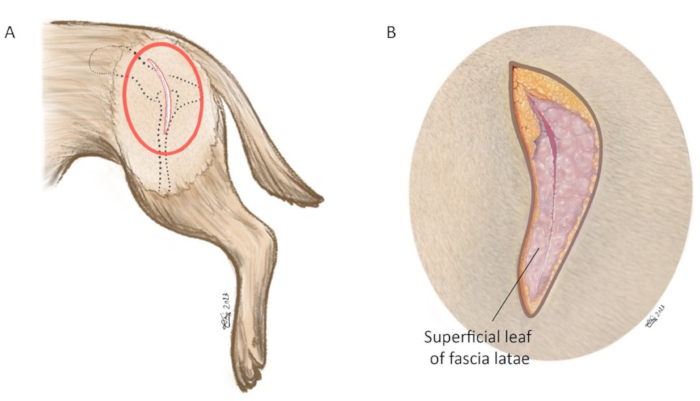
Figure 6: Schematic illustration of skin incision. (A) Red oval marks the area in which the skin incision is made. (B) Magnification of red circle in (A). The skin incision is made using a #10-blade centered on the tip of the greater trochanter aiming at the cranial dorsal iliac spine. The incision length is approximately 8-15 cm. In the magnified image, the superficial leaf of fascia latae is incised along the cranial muscle border of the biceps femoris muscle. Orientation: left is cranial, top is dorsal. Please click here to view a larger version of this figure.
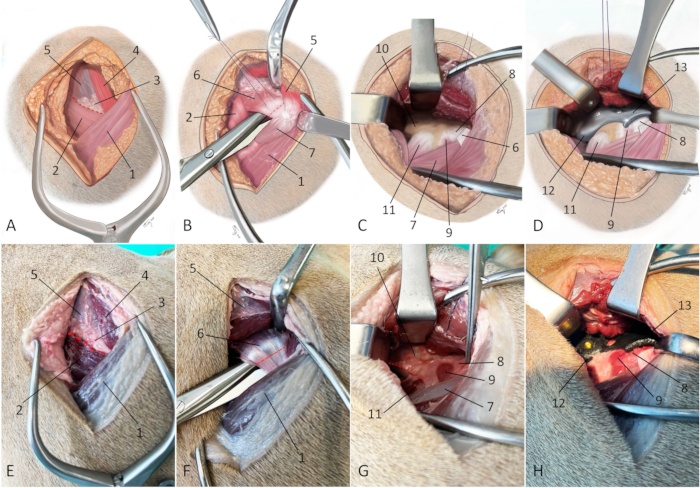
Figure 7: Schematic illustrations and photographs of an embalmed cadaver depicting the surgical approach for 3DHIP implantation. (A–D) Schematic illustrations and (E–H) photographs of an embalmed cadaver depict the surgical approach for 3DHIP implantation. (A and E) The red dotted line marks the line of the incision through the intermuscular septum between the superficial gluteal muscle, middle gluteal muscle, and the tensor fascia latae muscle. (B and F) Red dotted line marks the tenotomy site. The superficial and middle gluteal muscles are retracted dorsally to expose the deep gluteal muscle. Dissecting scissors are used to undermine the deep gluteal muscle near its insertion on the greater trochanter. A tenotomy is performed close (at 0.5-1 cm) to its insertion on the bone. (C and G) Adequate exposure for 3DHIP implant placement requires freeing the deep gluteal muscle from the joint capsule and lateral surface of the iliac body and partially freeing the iliacus muscle and rectus femoris muscles from the caudoventral border of the ilial shaft (red dotted line). (D and H) The 3DHIP implant is placed outside the capsule of the hip joint. For accuracy and ease of positioning, the ilium flange of the attachment part of the implant is placed under the ventral border of the exposed caudoventral iliac shaft. Orientation: left is cranial, top is dorsal. 1) biceps femoris muscle, 2) tensor fascia latae muscle, 3) fatty triangle, 4) superficial gluteal muscle, 5) middle gluteal muscle, 6) deep gluteal muscle/tendon, 7) vastus lateralis muscle, 8) hip joint capsule, 9) articularis coxae muscle, 10) caudal part of iliac body, 11) rectus femoris muscle, 12) ilium flange of the implant, and 13) rim extension part of the implant. Please click here to view a larger version of this figure.
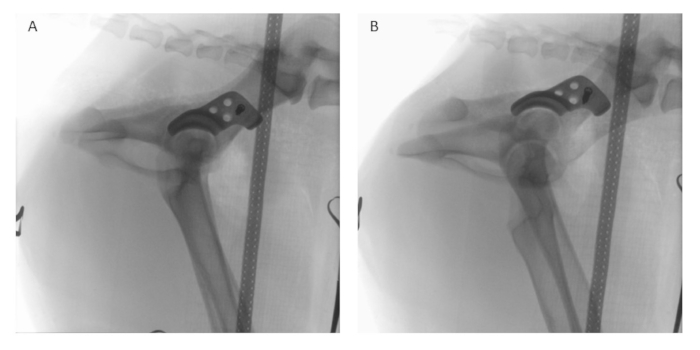
Figure 8: Intraoperative fluoroscopy. After implant positioning and temporary fixation with one locking screw, intraoperative fluoroscopy is performed in (A) lateral and (B) latero-oblique views using a digital image intensifier to assess and compare the positioning of the implant to the preoperative planning. Please click here to view a larger version of this figure.
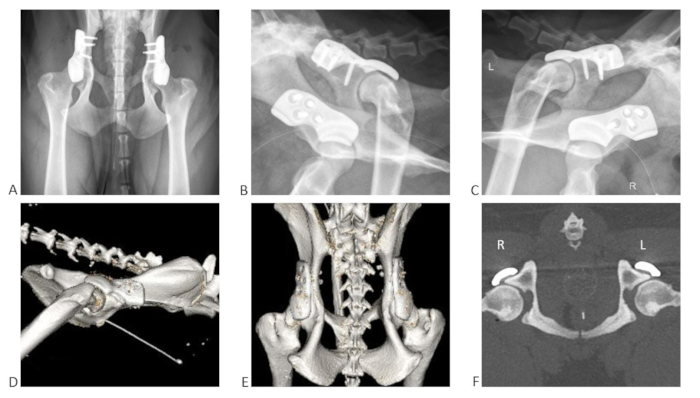
Figure 9: Examples of postoperative radiographs in three planes and postoperative CT scan after single-stage bilateral 3DHIP implant surgery in one dog. (A) Radiograph ventrodorsal view; (B) radiograph right latero-oblique view; (C) radiograph left latero-oblique view. 3D reconstruction from post-operative CT in lateral view showing the (D) right hip and (E) dorso-ventral view. (F) Postoperative CT of both hips in the transverse plane with a slice thickness of 5 mm. The 3DHIP implants were fixed with four locking screws on each side. Please click here to view a larger version of this figure.
| Outcome measurements | Preoperatively | Immediated postoperatively | 1.5 months | 3 months | p-value |
| NA (◦) | 87 ± 13a | 134 ± 19b | – | 131 ± 20b | <0.001* |
| LFO (%) | 22 ± 15a | 81 ± 16b | – | 76 ± 19b | <0.001* |
| PC (%) | 33 ± 17a | 79 ± 21b | – | 77 ± 20b | 0.002* |
| HCPI (%) | 31.44 ± 11.9a | – | 20.39 ± 10.09b | 17.69 ± 10.8b | <0.001** |
Table 1: Short-term results (Mean ± SD) of radiographic measurements using coronal CT and pain-related owner questionnaire using Helsinki Chronic Pain Index in dogs with hip dysplasia that underwent 3DHIP implantation. This table was modified from Kwananocha et al.18. HCPI (%) = 100% × total index score/maximum possible index score of the answered questions. a,bp-value < 0.05 from Bonferroni, p-value* from repeated measure analysis, p-value** from generalized linear mixed model. Abbreviations: NA = Norberg angle; LFO = linear percentage of femoral head overlap; PC = percentage of femoral head coverage; SD = standard deviation; HCPI = Helsinki Chronic Pain Index.
Supplementary Video S1: Direct postoperative weight-bearing allowed with only short leash walks on a slip-resistant floor from the day after surgery. Please click here to download this video.
