The pelvic examination is performed for diagnostic, screening and treatment purposes as a part of gynecologic, obstetric and sexual health care. A comprehensive pelvic exam includes assessment of the external genitalia-which will be discussed in this video, followed by examination of the vagina and cervix with a speculum-to be covered in the video titled Pelvic Exam Part II; and a bimanual evaluation of the pelvic organs-reviewed in Part III of this series.
Here, we will first discuss how to introduce this exam to a patient. Subsequently, we will review the steps for external genitalia assessment, which includes inspection as well as digital evaluation.
Before discussing the physical examination steps, let’s review how to introduce this exam to a patient, the set-up necessary and a few general considerations. The pelvic exam can feel invasive to patients, so it is important to do everything possible to make them feel comfortable and empowered, rather than vulnerable. Right at the start you must establish an expectation of comfort and ask your patient to communicate their questions and concerns during the visit. If the patient has had a pelvic exam before, you should inquire about that experience. Reassure the patient by saying something like “Dialogue”.
Before beginning with the procedure, it is important that you introduce and summarize the exam, “Dialogue”. Remember, that while it is always important to avoid extremely clinical language, certain colloquial words can cross the line from being caring to being overly intimate during this exam. It is helpful to avoid the words “touch” and “feel,” which can feel sexualized in this context; instead, the words “assess,” “check,” “inspect,” or “examine” should be used. The words “bed” and “sheet” should be avoided, and “table” and “drape” should be used instead. Also, a clinician should use the word “footrests” rather than “stirrups”. It’s a good idea to avoid telling patients to “relax” because it’s a hard order for a patient to follow when they’re anxious. Practicing clinicians often utilize a chaperone for their own or the patient’s comfort, and based on institutional policies. However, in this video demonstration we will not be using a chaperone. Ask the patient to change into a gown and specify how they should dress-underwear off, and gown open in the back. Also provide the patient with a drape to place over their lap and step out of the room to give them privacy.
Set up all the supplies you will need, before beginning the exam. If you will be using lubricant at any point make sure to squeeze it onto a clean area before beginning, as you cannot touch the packets or bottle once you are wearing gloves. Make sure to have a trashcan, a working light, and a stool near the exam table.Give the patient a hand mirror so they can follow along with the exam and say, “Dialogue”. Pull out the footrests and ask the patient to place their feet over them. Raise the back of the exam table to 45-60° and ask the patient to sit back. This modified lithotomy position allows the patient to see the examiner and facilitates the examination, as the patient’s internal organs sink into the pelvic basin making them much easier to assess.
After the patient is comfortable, wash your hands thoroughly. Sit down on the stool near end of the exam table, and put on gloves. Then, place the back of your hand on the end of the table over the drape and ask the patient to slide down until they can feel the back of your hand. Next, ask them to extend their knees sideways. Now, using both your hands, fold the drape up toward the patient’s pubic bone. Then, request the patient to hold it in place using their free hand. Next, ask the patient to bring the mirror next to one of their knee. Place two fingers near, but not touching, the patient’s vulva and say, “Dialogue”. To put the patient at ease and avoid muscle spasm, establish a non-invasive contact first, “Dialogue”.
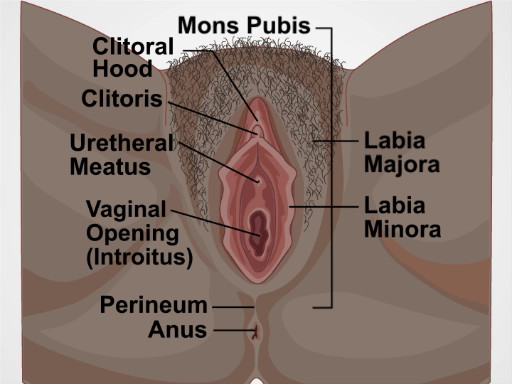
The structures evaluated during visual inspection include: mons pubis, which overlies the pubic symphysis, the labia majora that appear as rounded folds and are composed of adipose tissue, and more internally, the labia minora, the clitoris and the clitoral hood. Between the labia minora, there are two opening: the uretheral meatus and the vaginal opening, known as the introitus. The term perineum describes the tissue between the introitus and the anus. During the exam visually assess for the following: the pattern of hair growth, rashes, lesions, moles, masses, and discharge. Also look for potential signs of domestic violence such as scarring, burns, or bruising; signs of female genital mutilation; hemorrhoids; skin tags; fissures; and other irregularities.
To view these structures, position the index and middle fingers of dominant hand in a “peace” sign and keep the other fingers tucked. With the pads of your index and middle fingers, separate the labia minora and majora on one side to inspect the entirety of the sulcus. Keep your hand low and take care to avoid accidental extraneous contact with the clitoris by keeping fingers that aren’t being used tucked in. Using the same two fingers, separate the labia minora to view the vaginal introitus and urethral opening. Then, rotate your wrist up and use the back of the two fingers to retract the clitoral hood and view the clitoral shaft. Lastly, make a fist, and using the back of your fist pull away one buttock to view the anus. If you notice a mole or freckle, point it out to the patient and let them know they should regularly check it for changes, just as they would with moles elsewhere on their body.
The next part of the exam is the digital assessment of the vestibular glands, the vagina and the cervix. To start, first lubricate the turn your dominant index finger. Let the patient know you will be placing a finger in their vagina. In palm down position, place the lubricated finger into the vaginal introitus to just beyond your first knuckle. Then gently pinch the tissue between your thumb and the inserted finger at five and seven o’clock positions to assess the Bartholin’s glands located posteriorly. Watch the patient’s face for signs of discomfort and note if you feel any palpable masses.
Next, apply posterior pressure and rotating your palm up. Then using the thumb and middle finger separate the labia minora to visually inspect the urethral meatus and the openings of the paraurethral or Skene glands-located bilaterally next to the urethral meatus. Note the signs of inflammation and presence of discharge. Express the Skene’s glands by tapping gently upward with your index finger at one and eleven o’clock positions. If the glands are infected they discharge into the urethra, so finish by making a gentle beckoning motion at twelve o’clock to check if the glands release any discharge, which is absent in this case.
Then, release the labia and insert your finger farther to locate the cervix; assess its depth and direction. This will help you choose the correct speculum size and also help you decide where to angle the speculum during the other part of the exam.If you can easily locate the cervix while sitting down, the patient may need a short speculum. If you cannot easily locate the cervix, then you might have to stand up and the use a medium or a longer speculum.
Next, perform digital vaginal assessment. Slide your index finger halfway out and then rotate to palm down position. Subsequently, insert your middle finger by placing it over the top of your index finger and then place them side-by-side.Now, drop your wrist and pull down toward the perineum to make space above your fingers. Next, ask the patient to perform the Valsalva maneuver by bearing down as if having a bowel movement and assess cystocele, which refers to anterior bladder prolapse. Following that, lift your wrist up to apply anterior pressure toward the bladder until space underneath the fingers can be seen. Again, ask the patient to bear down while assessing for rectocele denoted by rectal herniation into the back wall of the vagina.
Next, lower your wrist so the fingers are flat and centered and gently separate them. This will also help in choosing the right speculum for the following part of this exam. If you’re having difficulty in separating your fingers, the exam should be performed with a small size speculum.Finally, assess the tone of the pubococcygeal muscle by asking the patient to squeeze around your fingers as if they are stopping the flow of urine. This maneuver is called the Kegel’s exercise. A firm squeeze represents a healthy and toned pelvic floor. Remove your fingers and discard the gloves. This completes the first part of the pelvic exam.
You’ve just watched JoVE’s video on the approach to the pelvic examination and assessment of the external genitalia. In this video, we reviewed how to introduce the pelvic exam to a patient, demonstrated the inspection of the external genitalia, and showed the steps to be performed during the digital assessment of the cervix and vagina. As always, thanks for watching!