The operative setup and midline laparotomy is shown in Figure 1. The laparotomy incision should be curved to avoid the urogenital opening (Figure 1B). When setting up the retractor, attach the post for the Omni or Bookwalter retractor to the left, inferior corner of the table. Ideal retraction includes two retractor blades for the right abdominal wall, two for the left abdominal wall, and 1-2 for the right colon and small bowel wrapped in a sterile towel (Figure 1C). Body wall, splanchnic, or malleable retractor blades can be used, depending on the availability of an assistant and operator preference. If an Omni or Bookwalter retractor is not available, 1-2 self-retaining Balfour retractors can be used to retract the abdominal wall on either side. An assistant can then apply retraction to the right colon and small bowel wrapped in a sterile towel.
The retroperitoneal dissection carried out in Figure 2 can be performed with a mix of blunt and sharp dissection. While it is important to obtain circumferential control of the infrarenal IVC and aorta, this dissection does not need to be continued down to the bifurcation. The intrathoracic portion of the procedure is the most technically challenging (Figure 3), as injury to the intrathoracic or retrohepatic IVC can cause significant bleeding and obscure the operative field. When identifying the descending thoracic aorta, bluntly separate the aorta from the esophagus using your thumb and index finger. To avoid the avulsion of small intercostal arteries and subsequent bleeding, circumferential control is not essential as long as the descending thoracic aorta is accessible with a clearly defined space to accommodate an aortic clamp.
Cannulation of the infrarenal aorta is performed using the Seldinger technique (Figure 4). This can be done with the infrarenal aorta clamped proximally and distally (Figure 4A), or directly without clamping. Be careful not to insert the needle through the back wall of the aorta. A larger sheath can also be used if the aorta is of sufficient size. It is important to purge air from the IV extension tubing and connect the IV tubing from the UW solution to the 10Fr sheath in a sterile fashion. Ensure the IV channel is open, although flow will not initiate until the aorta is clamped (Figure 4B). When making the venotomy in the infrarenal IVC, it is important for the primary surgeon to securely grip the IVC using DeBakey forceps, so as not to lose the site of the venotomy and have a large blood volume pour into the operative field. A venotomy away from the pancreas, with the prompt placement of pool suction, maintains a bloodless operative field with clear tissue planes for the pancreatectomy (Figure 4C). Initial drainage will be dark venous blood, but this will lighten as the pig is exsanguinated and UW solution is perfused through the viscera. Be sure to use a large suction canister for this portion of the procedure.
The viscera, and in particular, the pancreas, will become increasingly pale as the UW solution is perfused (Figure 5A). The pancreatic duct can be identified by following the course of the duodenal lobe into the duodenum. The duct should be divided between two silk ties to avoid contamination with enteric contents (Figure 5B). While the pancreatic parenchyma should appear pale and bloodless, the remaining connective tissue surrounding the pancreas should be cleaned prior to islet isolation (Figure 5C).
The harvested pancreas can then undergo a multi-step islet isolation and purification process (Figure 6). Figure 7A shows the representative islet size distribution after the islet isolation and purification process. Figure 7B shows purified islets using brightfield microscopy, and after live/dead staining, with green and red staining representing viable and non-viable islet cells, respectively. Islet yield and purity can be evaluated using an islet cell counter. Representative yields are provided from three independent porcine pancreatic isolations are summarized in Figure 7C.
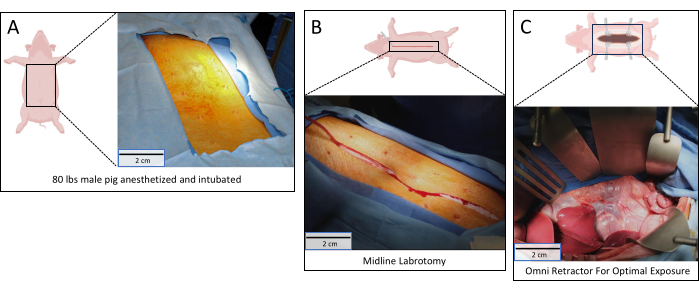
Figure 1: Operative setup. (A) Pig positioned in supine position with the abdomen sterilely prepped; (B) Midline laparotomy made from xiphoid to pubis; (C) Retroperitoneum exposed with Omni retractor in place. Scale bars = 2 cm. Please click here to view a larger version of this figure.
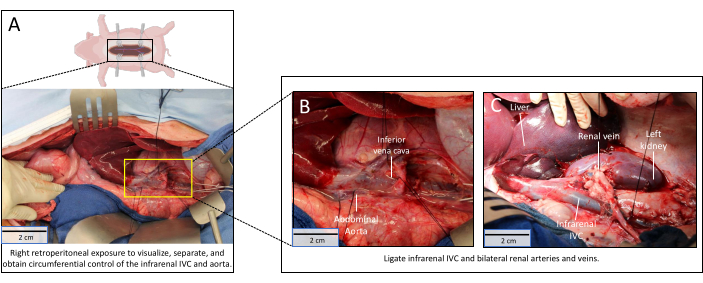
Figure 2: Retroperitoneal dissection. (A) Retroperitoneum dissection complete with circumferential control of the infrarenal IVC and renal veins. The yellow rectangle is magnified in Figure 2B; (B) Magnified image of infrarenal IVC and renal veins; (C) Renal veins tied off. Scale bars = 2 cm. Abbreviation: IVC = inferior vena cava. Please click here to view a larger version of this figure.
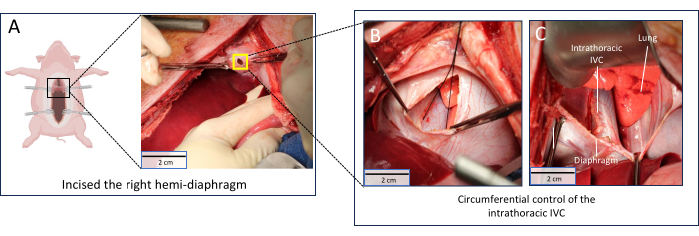
Figure 3: Obtaining supraceliac control. (A) Right hemidiaphragm incised. The yellow square is magnified in Figure 3B; (B) Extension of right hemidiaphragm incision to expose intrathoracic IVC and descending thoracic aorta; (C) Circumferential control of intrathoracic IVC obtained. Scale bars = 2 cm. Abbreviation: IVC = inferior vena cava. Please click here to view a larger version of this figure.
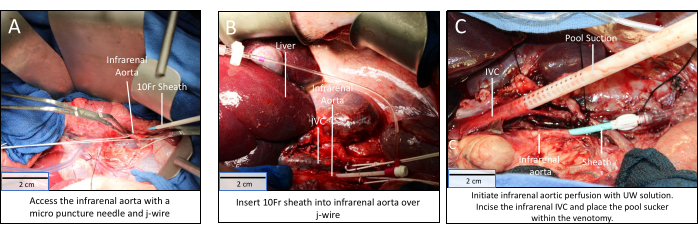
Figure 4: Infrarenal aortic cannulation, visceral isolation, and perfusion. (A) Proximal and distal control of the infrarenal aorta obtained; (B) 10Fr sheath placed in the infrarenal aorta by Seldinger technique; (C) Visceral perfusion via the infrarenal aortic sheath and drainage via venotomy and pool sucker in infrarenal IVC. Scale bars = 2 cm. Abbreviation: IVC = inferior vena cava. Please click here to view a larger version of this figure.
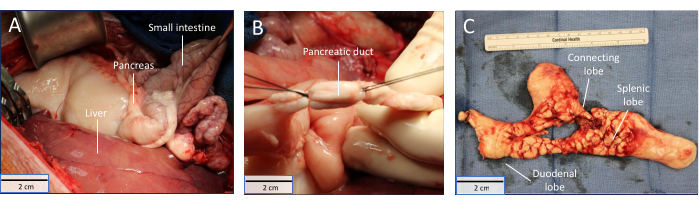
Figure 5: Total pancreatectomy. (A) Viscera becoming paler during perfusion; (B) pancreatic duct isolated; (C) Explanted porcine pancreas. Scale bars = 2 cm. Please click here to view a larger version of this figure.
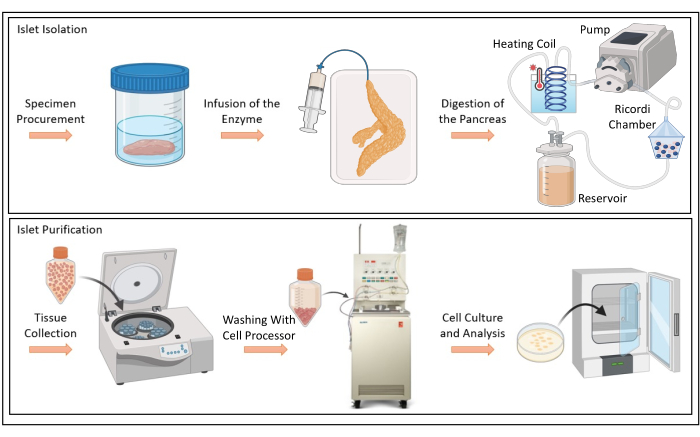
Figure 6: Islet isolation and purification. Schematic depiction of infusion of enzyme solution, digestion of porcine pancreas, tissue collection, cell washing with Cell Processor, and cell culture and analysis. Please click here to view a larger version of this figure.
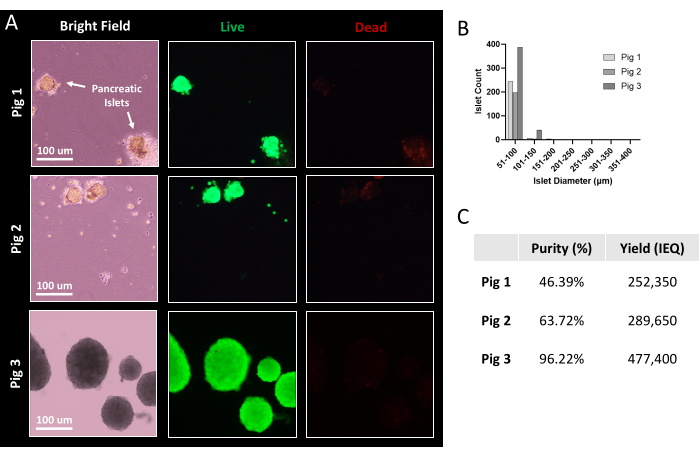
Figure 7: Representative islet viability and yield after purification. (A) Porcine islets after magnified bright-field imaging and live/dead staining. Green demonstrates live cells; red demonstrates dead cells. Scale bars = 100µm (B) Histogram distribution of porcine islet size following purification. (C) Table indicating islet purity and yield from three porcine pancreatic islet isolations. Abbreviation: IEQ = islet equivalent, the standard unit for islet quantification. Please click here to view a larger version of this figure.
