In Vivo Gene Transfer to the Rabbit Common Carotid Artery Endothelium
Summary
This method is to introduce a transgene into the endothelium of rabbit carotid arteries. Introduction of the transgene allows the assessment of the biological role of the transgene product either in normal arteries or disease models. The method is also useful for measuring activity of DNA regulatory sequences.
Abstract
The goal of this method is to introduce a transgene into the endothelium of isolated segments of both rabbit common carotid arteries. The method achieves focal endothelial-selective transgenesis, thereby allowing an investigator to determine the biological roles of endothelial-expressed transgenes and to quantify the in vivo transcriptional activity of DNA sequences in large artery endothelial cells. The method uses surgical isolation of rabbit common carotid arteries and an arteriotomy to deliver a transgene-expressing viral vector into the arterial lumen. A short incubation period of the vector in the lumen, with subsequent aspiration of the lumen contents, is sufficient to achieve efficient and durable expression of the transgene in the endothelium, with no detectable transduction or expression outside of the isolated arterial segment. The method allows assessment of the biological activities of transgene products both in normal arteries and in models of human vascular disease, while avoiding systemic effects that could be caused either by targeting gene delivery to other sites (e.g. the liver) or by the alternative approach of delivering genetic constructs to the endothelium by germ line transgenesis. Application of the method is limited by the need for a skilled surgeon and anesthetist, a well-equipped operating room, the costs of purchasing and housing rabbits, and the need for expertise in gene-transfer vector construction and use. Results obtained with this method include: transgene-related alterations in arterial structure, cellularity, extracellular matrix, or vasomotor function; increases or reductions in arterial inflammation; alterations in vascular cell apoptosis; and progression, retardation, or regression of diseases such as intimal hyperplasia or atherosclerosis. The method also allows measurement of the ability of native and synthetic DNA regulatory sequences to alter transgene expression in endothelial cells, providing results that include: levels of transgene mRNA, levels of transgene protein, and levels of transgene enzymatic activity.
Introduction
The goal of this method is to introduce a transgene into the endothelium of rabbit common carotid arteries. Introduction of the transgene allows the assessment of the biological role of the transgene product both in normal arteries and in rabbit models of human arterial disease. Overexpression of the transgene in disease models can reveal whether the transgene (and its protein product) show promise as therapeutic agents1,2,3,4. Inclusion of cis-acting regulatory elements in the transgene expression cassette enables assessment of the activity of these elements in arterial endothelium in vivo5,6. Knowledge of the activity of specific cis-acting regulatory elements can be used to design more-active expression cassettes and to probe mechanisms of gene regulation in large artery endothelium in vivo7.
Rabbits are a valuable model for various aspects of human vascular physiology and disease. Rabbits share many vascular features with humans. For example, baseline hematological values, hemostatic regulation, and vascular longitudinal tension are similar between rabbits and humans8. Rabbit models of vascular diseases replicate key features of many human diseases including: aneurysms (similar geometric and flow characteristics)9, vasospasm (similar response to endovascular treatment)10,11, and atherosclerosis (intimal plaques with similar features including a core rich in lipid, macrophages, and smooth muscle cells in a fibrous cap)12,13. Accordingly, rabbit models have been developed for many vascular diseases such as thrombosis, vasospasm, aneurysm, diabetes, vascular graft stenosis, and atherosclerosis8,13,14,15,16.
For researchers choosing among animal models of vascular physiology and disease, the rabbit has several advantages. Compared to rodents, the larger vessels of rabbits allow easier surgical manipulation, use of endovascular devices, and a larger amount of tissue for quantitative measurements. Rabbits are much closer phylogenetically to primates than are rodents17, and the greater genetic diversity of outbred rabbits better approximates the genetic variability of humans. Genetic diversity is particularly important for preclinical studies, which-by their nature-aim to develop therapies that can be applied to the genetically diverse human population. As with many if not all other model species, rabbit genes are easily cloned or synthesized because the rabbit genome has been sequenced with high coverage (7.48x) [http://rohsdb.cmb.usc.edu/GBshape/cgi-bin/hgGateway?db=oryCun2]. Compared to other large animal models (such as dogs, pigs, or sheep), rabbits are relatively inexpensive to purchase and house and they are easier to breed and handle. Specific vascular disease models in rabbits each have their own advantages and shortcomings as models of human disease that are beyond the scope of this manuscript8,12,18. An investigator should review these advantages and shortcomings to determine if the rabbit is the best model for answering a specific experimental question.
Introduction of deoxyribonucleic acid (DNA) regulatory sequences into endothelial cells in vivo enables investigation of the activity of these sequences in a complex physiologic environment. In vitro studies in transfected endothelial cells can be useful for the initial assessment of DNA regulatory sequences; however, expression levels in tissue culture models are sometimes not reproduced when the studies are repeated in vivo5,19,20. In vitro systems can also be useful for exploring basic pathways of protein signaling and endothelial physiology as well as communication between cultured vascular cells; however, more-complex pathways or regulatory networks that are influenced by complex populations of neighboring vascular cells or the immune system are best studied in an in vivo system6,20. The method described herein provides a platform for exploring regulation of transgene expression in the endothelium within the context of an intact vessel, with or without disease. The in vivo system also permits investigation of physiological and pathological cellular crosstalk and identification of contributions of the immune system to regulation of gene expression6.
Germ-line transgenesis (especially in mice) is an alternative approach for directing transgene expression to endothelial cells. This approach can provide life-long transgene expression, with endothelial targeting mediated by specific promoter or regulatory regions21,22. However, the generation of transgenic mice is time-consuming and expensive, several transgenic lines must be often tested to ensure targeting of the transgene to the desired cell type and achievement of adequate transgene expression levels, and experimental results in murine systems can be strain-dependent. Murine transgenic models with endothelial-targeted transgenes have many advantages: there is no need to perform surgery on every experimental animal in order to achieve transgenesis, experimental mice can be bred with numerous other available transgenic mice in order to test genetic and phenotypic interactions, and there is a wide selection of antibodies that react with murine proteins, facilitating characterization of phenotypes. However, targeting of transgenes to the endothelium via the germ line typically results in transgene expression throughout the vasculature,22 making it difficult to determine the site at which the transgene product is acting. This is especially true when the transgene product is secreted, because a transgene product secreted by endothelial cells throughout the vasculature could have biological activity at any number of sites within an animal. Although the method described in this manuscript requires technical expertise and specialized facilities, it can be less time consuming and less expensive than developing an endothelial-specific transgenic mouse line. It allows for the assessment of the function of a protein selectively in endothelial cells of a segment of large artery, and it permits use of the contralateral common carotid as a paired control (eliminating systemic factors that can vary among experimental animals-for example, blood pressure or cholesterol levels-as uncontrolled variables).
Gene therapy is a promising approach for the treatment of vascular diseases, particularly chronic diseases, because a single application can provide sustained or possibly life-long expression of a therapeutic gene23. The therapeutic promise of gene therapy has been explored in animal models of somatic gene transfer, often targeting the liver24,25, which is a relatively easy target because many blood-borne viral vectors are hepatotropic. However, to have an effect on vascular disease, gene therapy targeted to the liver must achieve systemic overexpression of proteins. This typically requires large doses of vector, which can be toxic or even fatal26. Moreover, increased systemic levels of a protein raise the risk of off-target side effects, which could complicate or even obscure interpretation of experimental results. Local gene therapy targeting vascular endothelium as described in this manuscript could avoid systemic side effects because the infused vector is not widely disseminated beyond the transduced arterial segment, and local vascular effects can be achieved without changes in systemic plasma levels of protein.27 In addition, a far lower amount of vector is needed to transduce an arterial segment than is needed to achieve robust hepatic transduction. Transgene expression from the liver has been reported to decline over time, probably due to cell turnover, requiring repeated dosing if high-level transgene expression is to be maintained.28 In contrast, the low turnover rate of the endothelium provides stable expression for at least 48 weeks in chow-fed rabbits and for at least 24 weeks in atherosclerotic lesions of cholesterol-fed rabbits.1,27
To determine if this method of gene transfer to rabbit common carotid endothelium is appropriate, the advantages and disadvantages (Table 1) should be considered in the context of the specific research goals. Advantages of this method include: outbred rabbits are better representative of human genetic diversity than are inbred mice (important for preclinical work); rabbits provide larger vessels for easier manipulation and more tissue for analysis; the method can achieve endothelium-targeted transgene expression far more quickly than does germ-line endothelial targeting in transgenic mice; vector dose can be easily adjusted to model variable levels of transgene expression; processes specific to large-artery endothelium can be investigated; and local vascular transgenesis allows the opposite carotid in the same animal to be used as a control, eliminating systemic factors as uncontrolled variables. Disadvantages include: special facilities and expertise are required; fewer genetically modified backgrounds on which to experiment are available in rabbits than in mice; and there is a less extensive selection of antibodies to rabbit versus mouse proteins (for immunodetection of transgene protein and other antigens that may be important in interpreting experimental results).
Protocol
All methods described here were approved by the University of Washington Office of Animal Welfare and associated Institutional Animal Care and Use Committee (IACUC), and were completed in accordance and compliance with all relevant regulatory and institutional guidelines.
Note: Gene transfer to rabbit common carotid arteries is performed on rabbits by a surgeon with the aid of an anesthesiologist or assistant.
1. Gene transfer to rabbit common carotid arteries: Pre-operation
- Anesthetize the rabbit. Weigh the rabbit. Combine 30 mg/kg ketamine and 2 mg/kg xylazine into a syringe. Inject ketamine/xylazine intramuscular (IM) in the paraspinous muscles to induce anesthesia.
- While waiting for rabbit to become anesthetized, prepare the preparation room and operating room (OR) tables.
- In the OR preparation room: place the ophthalmic ointment and the fentanyl patch within reach of the preparation table; set up hair clippers and a vacuum for shaving the rabbit's neck and ear; set aside an alcohol prep pad, a 24G x ¾" catheter, an injection port, and surgical tape to secure the intravenous line (IV) in the rabbit's ear vein.
- In the OR: set up the monitoring equipment and position the probes [electrocardiogram (EKG), oxygen saturation (SpO2), temperature] on the OR table; prepare oxygen and isoflurane; tie gauze strip to the face mask to secure it to the rabbit and place the mask on the head end of table.
NOTE: The gauze strips tied on the face mask should have 2 tails of about 45 cm each. - Turn on the warming water blanket on the OR table. On top of water blanket, position a rolled towel for neck support and a dispersive electrode plate (later placed under rabbit's back).
- Set up the OR IV pump with 100 mL of a saline IV bag with an 18-19G needle attached and set the flow rate to 10 mL/h per kg.
- Combine 1 mL of lidocaine HCl (2% stock solution) and 1 mL of bupivicaine HCl (0.5% stock solution) in a syringe, to be used as a local analgesic.
- When rabbit is fully anesthetized, prepare the rabbit for surgery.
NOTE: Check for the lack of a pedal reflex (pinch a toe; look for limb withdrawal) to ensure anesthetic depth, and continue to monitor the pedal reflex throughout the surgery.- Apply ophthalmic ointment to eyes. Remove stool from the rabbit's rectum by pressing with gloved fingers on the lower anterior abdomen (above rectum) and moving fingers towards the anus. This will allow for later placement of a rectal temperature probe.
- Shave the anterior neck from the sternal notch to the edge of the mandible while using a vacuum to keep the area clean. Also shave both ears for the IV placement and the fentanyl patch attachment, and shave a left rear middle toe for the pulse-oximetry probe.
NOTE: The protocol assumes that the surgeon is on the rabbit's right side for the entire procedure. If the OR setup places the surgeon on the opposite side, reverse sides in this step to keep the wires and IV opposite of the surgeon. The sides of future steps should also be switched as needed. - Wipe the left ear with an alcohol prep pad, place an 24G IV catheter into the left ear vein, cap with the injection port, and tape the catheter/port to the rabbit's ear to secure it. Apply a fentanyl patch (25 µg/h) to the rabbit's right ear.
- Transport the rabbit into the OR and place supine on the operating table with a rolled neck support towel under the rabbit's neck just below the head. Gently extend the rabbit's neck until it is straight and approximately horizontal.
- Hook the rabbit up to the face mask with O2 on at 1 L/min, and start isoflurane administration. Secure the mask by wrapping the ends of the gauze strip tied to the mask around the neck support towel under the rabbit. Adjust isoflurane (typically 1 – 2%) as needed (based on heart rate, respiratory rate, and pedal reflex) to maintain proper anesthesia for the remainder of the procedure.
- Ensure that the dispersive electrode plate is centered under the rabbit's back. Place the temperature and pulse-oximeter probes and apply the EKG leads to the rabbit.
- Hook up IV saline to the catheter port in the rabbit's ear, starting the saline pump at 10 mL/h per kg.
NOTE: After 1 h, the saline pump can be reduced to 5 mL/h per kg. - Restrain the rabbit's front legs by loosely tying them to the table. Optionally, place a small plastic table over the rabbit to protect the rabbit from being subjected to chest/abdominal pressure from the surgeon leaning on rabbit's chest/abdomen.
NOTE: The small table may help prevent forced regurgitation of abdominal contents. - Inject 2 mL of previously prepared lidocaine (2% stock)/bupivacaine (0.5% stock) (50/50 mix) subcutaneously along the planned neck incision line for local anesthesia.
- Let the assistant prepare the surgical site with 3 alternating scrubs of chlorhexidine and isopropanol, and then a spray with betadine. Scrub, gown, and glove, following proper aseptic technique.
NOTE: The surgeon should be wearing 2x surgical loupes to aid with the first half of the surgery. During the survival surgery it is vital to maintain sterility of the surgeon and the surgical field. Only the assistant should handle any non-sterile items, and sterilized materials must be aseptically passed to the surgeon or placed on the draped instrument table. Sterile towels can be used by the surgeon to maintain sterility while manipulating non-sterile equipment such as the microscope.
2. Survival Surgery (Gene Transfer)
- Prepare instruments and sterile field.
- Let the assistant open the sterile drape pack containing a table drape, one paper drape for the rabbit, and several towels. Aseptically transfer the items to the surgeon.
- Drape the instrument table. Place the 6 sterile towels and the paper drape onto the draped table.
- With 4 towels, drape the rabbit's neck, leaving only the surgical site exposed (approximately 4 cm x 10 cm). Lay the paper drape over the rabbit.
- Let the assistant open the sterilized instrument pack and place aseptically onto the instrument table.
- Let the assistant open the following equipment and aseptically place onto the instrument table or hand to the surgeon: three 1-mL syringes (and one needle if the syringes are not already loaded with needles), one 20 mL syringe, one 21G needle, one 19G needle, 3-0 polyglycolic acid (PGA) suture, 5-0 PGA suture, 7-0 polypropylene suture, and two 24G IV-catheters.
- Secure the electrocautery cable to the rabbit drape using the 7.25" Kantrowitz Forceps and then drop the plug end off of the table. Let the assistant connect the cable to the electrosurgery unit and turn the power on.
- Fill a 20 mL syringe with sterile saline, drawn from an IV bag or vial held by the assistant. Use this saline as needed to keep exposed tissue moist during the procedure.
- Prepare one 1 mL syringe with 1 mL of Dulbecco's Modified Eagle Medium (DMEM, for washing the artery). For each carotid artery that will be transduced, 0.35 mL of diluted virus are needed. If the same virus is used for both sides, prepare one 1 mL syringe with virus diluted in DMEM to a volume of 0.7 mL. If different sides are receiving different viruses [for example a "Null" virus control on one side], prepare two 1 mL syringes, each with 0.35 mL of virus solution. For helper-dependent adenovirus, the virus concentration is 2 x 1011 viral particles (vp)/mL.
NOTE: Let the assistant prepare the virus. The surgeon draws up DMEM and virus suspension into sterile syringes. - Cut a hole in the drape. The size of the hole should be the same size as the surgical site on the rabbit's neck that is framed by the towels in step 2.1.3. Clamp the corners of the hole in the paper drape to the underlying towels that are draped over the rabbit's neck with the towel clamps.
- Isolate the common carotid arteries.
NOTE: 2x surgical loupes should be used for this part.- Cut the skin with an electrocautery along the midline extending approximately 7 – 9 cm cranially toward the mandible and clamp the skin open with towel clamps.
- Make a short lateral cut through the fascia with the electrocautery at the caudal end. Then insert the large scissors into the cut and bluntly dissect the fascia along entire midline. Cut the dissected fascia down the midline with electrocautery.
- With small dissecting scissors, dissect between the V-shaped muscles (sternocephalic muscle) and the sternohyoid muscle over the trachea, to expose the common carotid arteries, starting on the right side.
- Dissect the right common carotid artery free from surrounding tissues, dividing all branches, from base of neck caudally to the crossing of the pharyngeal nerve cranially. Use surgical silicon loops to aid in retracting the artery during dissection.
NOTE: Care should be taken to not disturb either the vagus nerve that runs parallel to the common carotid, or the smaller nerves that cross over the common carotid. - Ligate any large branches coming off the common carotid artery (1 – 2 per side) with 5-0 silk sutures prior to cutting the branch distally to free a 4 – 5 cm segment of the carotid. Cut ligated branches 1 – 2 mm away from the tie so that the tie does not slip off.
- Repeat dissection on the left side (steps 2.2.3 – 2.2.5).
- Infuse vectors into common carotid arteries.
NOTE: A surgical microscope (16X) is used as needed for performing arteriotomy, infusing vector/control solution, and arteriotomy repair.- Let the assistant remove the surgical loupes from the surgeon and move the surgical microscope into position. Drape a sterile towel over the microscope to allow manipulation of the microscope without contaminating the sterile field.
- Inject heparin [150 international units (IU)/kg] in the IV catheter and flush with 10 mL of saline.
- Returning to the isolated right common carotid, put two silk ties around the mid-portion of the mobilized carotid segment and tie a single overhand knot on each – without tightening them.
- Bend the 19G needle just above the bevel to approximately 80° using the large needle driver (do not bend the bevel; Figure 1).
- Clamp the artery at each end of the isolated segment with vascular clips, placing the cranial clip first to allow for artery filling, and then placing the caudal clip.
- Puncture the common carotid artery with the bent 19G needle just cranial to the caudal vascular clip, taking great care to not puncture the back or side walls. Advance the needle tip into the lumen and withdraw it twice to make sure arteriotomy completely traverses the artery wall. Then carefully withdraw the needle.
Notes: It is important to create an arteriotomy that penetrates all layers of the artery wall cleanly and does not dissect the artery wall (by passing axially through the adventitia and media). To accomplish this, the carotid should be punctured with the needle tip positioned as close as possible to a 90° angle against the artery wall (Figure 1). Carotid puncture at a 90° angle is aided by grabbing the artery by the adventitia with fine forceps and gently lifting the artery surface while pressing the tip of needle just caudal to the lift point. This maneuver also reduces the risk of hitting the back wall (Figure 1). - Unfold and bunch-up several gauze pads into a nest on which to lay the syringe used for the infusions. Place the nest on the rabbit's chest caudal to the incision.
- Put an IV-catheter on the syringe that contains DMEM-only (not too tight) and bend the catheter ~4 mm from the tip so that the bend holds at about 75° after it is released.
- Insert the IV-catheter in the artery up to the bend point and wash out all blood from the artery with DMEM (~ 0.25 mL x 2). For each wash, fill the artery with DMEM, and then remove residual DMEM from the vessel lumen by gently pressing on the artery with a gloved finger, beginning just caudal to the cranial vascular clip. While maintaining gentle pressure, slide the finger from cranial to caudal. The luminal contents will wash out via the arteriotomy.
- Keep the catheter in the artery and exchange the DMEM syringe for the syringe containing virus solution. Make sure that no air enters the catheter.
- Slide the silk ties down the artery so that they surround the artery at the location of the catheter tip, but do not tighten them.
- Infuse 0.03 mL of the virus solution to push the remaining DMEM out of the catheter and then empty the artery. Collapse it by again removing all fluid from the lumen with a finger, cranial to caudal (as in step 2.3.9).
- Tighten the two ties around catheter tip to seal the lumen. Infuse the virus solution (~ 0.25 mL; 2 x 1011 vp/mL for adenovirus) by pressing the syringe plunger gently until the artery is distended to physiological caliber.
NOTE: It is important that the artery expands to physiological caliber and remains distended during virus infusion. If not, the degree of gene transfer will drop significantly. - Gently lay the syringe down on the nest of the gauze.
- Place a 7-0 polypropylene suture in the common carotid adventitia just caudal of the cranial vascular clip to mark the cranial boundary of gene transduction
- After the virus-containing solution has been in the artery lumen for 20 min, remove the virus-containing syringe and replace it with an empty syringe. Aspirate the virus-containing solution gently until the vessel collapses and remove the syringe. Cut or undo the silk ties and gently remove the catheter.
NOTE: Cutting the ties very short aids in removing them. Remove the catheter carefully to avoid causing damage to the carotid endothelium. - Using the surgical microscope, close the arteriotomy with 7-0 polypropylene using an X-pattern (Figure 2).
- Make a first pass entering at the bottom-right of the arteriotomy and exiting the vessel at the bottom-left. Then cross the opening and make a second pass from top-right to top-left.
- Before tying down the suture, flush out the artery by very briefly releasing the cranial vascular clip. Blood will flow out of the arteriotomy when the clip is released, removing air and residual virus from the lumen.
- Pull the suture to gently close the arteriotomy and tie a suture with 2 square knots.
NOTE: Pulling the suture too tight will cause bunching of the tissue that will disturb flow, increasing the thrombosis risk and altering flow which can be an important uncontrolled variable in disease models.
- Release the cranial vascular clip, and then the caudal vascular clip using light pressure with gauze to stop any bleeding. If bleeding persists, continue pressure for 1 – 2 min. If the arteriotomy was properly closed, the bleeding always stops within this time frame.
- Let the assistant inject buprenorphine [0.02 mg/kg; subcutaneous (SQ)] at about this time to provide postoperative analgesia until fentanyl plasma levels become therapeutic.
NOTE: A second buprenorphine injection (0.02 mg/kg; SQ) may be needed 6 h after the first injection to maintain analgesia until fentanyl plasma levels become therapeutic. - Repeat virus infusion protocol on left side following steps 2.3.2 – 2.3.19.
- Wound closure
- Use a 5-0 PGA suture to close the midline fascia with a continuous suture.
- With a 3-0 PGA suture, close the skin with an intradermal pattern using a buried knot at both ends.
- Post-operative recovery and cleanup.
NOTE: The rabbit must be monitored continuously for proper oxygenation and body temperature while recovering from anesthesia. Recovery should take place in a calm, quiet environment.- Turn off isoflurane and oxygen flow and remove the face mask from rabbit.
- Unhook IV fluids but leave the IV port in place for emergency IV access.
- Take the rabbit to the recovery area and lay on its side in a cage with a warming water blanket turned on (or optionally a Bair Hugger heater).
- Give O2 by mask until the SpO2 is stable.
- Let the rabbit recover in a cage, flipping it to the other side every 15 min, until the rabbit can sit up on its hind legs and move around.
- When the rabbit is mobile, remove the IV from its ear before returning to the cage.
Note: Do not return the rabbit to the company of other animals until it is fully recovered from anesthesia.
- Dispose of anything that had contact with the vector or was in the operative field, following appropriate biohazard and sharps waste protocols.
3. Gene transfer to rabbit common carotid arteries: Post-operative Care
- Assess the rabbit's overall condition daily after surgery, checking for wound healing, evidence of infection, appetite, respiration, and signs of pain.
- Check the rabbit's ear position (ears down can be a sign of pain or distress, especially when coupled with an untidy appearance). Check that the rabbit remains mobile and active. Check the rabbit for normal respiration without stridor. Check that the wound is clean, dry and intact. Check the rabbit for a normal body temperature. Consult veterinary services if the rabbit is not mobile and active, with normal body temperature, a tidy appearance, a clean wound, and normal respiration.
- Check for normal food intake and evidence of fresh stool and urine.
NOTE: Food intake may be decreased following surgery, but should return to normal within 2 days; provide supplemental food as needed.
- Remove the fentanyl patch on post-operative day 3.
NOTE: Buprenorphine can be administered as needed for post-operative pain that is not managed by the fentanyl patch, or in case the fentanyl patch is removed early.
4. Terminal Harvest Surgery: Pre-operation
- Anesthetize the rabbit. See sections 1.3 and 1.3.5 regarding achievement and maintenance of anesthesia.
- Weigh the rabbit. Combine 30 mg/kg ketamine and 2 mg/kg xylazine into a syringe. Inject ketamine/xylazine IM in the paraspinous muscles to induce anesthesia.
- Prepare the preparation room and OR tables while waiting for the rabbit to become anesthetized.
- In the OR preparation room: setup hair clippers and a vacuum for shaving the rabbit's neck and ear.
- In the operating room: setup monitoring equipment and position the probes (SpO2, temperature) on the OR table; prepare oxygen and isoflurane; tie a gauze strip to the face mask to secure it to the rabbit and place the mask on the head end of table.
NOTE: The gauze strips tied on the facemask should have 2 tails of about 45 cm each. - Turn on warming water blanket on the OR table. On top of the water blanket, position a rolled towel for neck support and a dispersive electrode plate (later placed under rabbit's back).
- Combine 1 mL of lidocaine HCl (2% stock) and 1 mL of bupivicaine HCl (0.5% stock) (50/50 mix) in a syringe as a local analgesic.
- When the rabbit is fully anesthetized, prepare the rabbit for surgery.
- Remove stool from the rectum, as described in 1.3.1, to allow for later placement of a temperature probe.
- Shave the rabbit from the sternal notch to the angle of the mandible while using a vacuum to keep the area clean. Also shave the left rear middle toe for the pulse-oximetry probe.
NOTE: The protocol assumes that the surgeon will be on the rabbit's right side. If the OR setup will place surgeon on the opposite side, reverse sides in this step to keep the wires opposite of the surgeon. The sides of future steps should also be switched as needed. - Transport the rabbit into the OR and place supine on the operating table with a rolled neck support towel under the rabbit's neck just below the head. Gently extend the rabbit's neck until it is straight and approximately horizontal.
- Hook the rabbit up to face mask with O2 on at 1 L/min, and start isoflurane administration. Secure the mask by wrapping the ends of the gauze strip tied to the mask around the neck support towel under the rabbit. Adjust isoflurane (typically 1 – 2%) as needed to maintain proper anesthesia for the remainder of the procedure.
- Ensure the dispersive electrode plate is centered under rabbit's back. Place temperature and pulse-oximeter probes.
- Restrain the rabbit's front legs by loosely tying them to the table.
NOTE: Optionally, place a small plastic table over rabbit to protect the rabbit from being subjected to chest/abdominal pressure from the surgeon leaning on rabbit's chest/abdomen. The goal here is to prevent forced regurgitation of abdominal contents. - Inject 2 mL of lidocaine (2% stock solution)/bupivacaine (0.5% stock solution) (50/50 mix; from step 2.4) subcutaneously along the planned neck incision line for local anesthesia.
- Spray the surgical site with betadine. Put on clean gloves for surgical procedure.
5. Terminal Surgery (Vessel Harvest)
- Prepare instruments and surgical field.
- Open a clean drape pack containing a table drape and one paper drape for the rabbit. Drape the instrument table.
- Open the instrument pack, place onto the instrument table, and arrange instruments. Place the following equipment onto the instrument table: one 20 mL syringe, and one 21G needle.
- Secure the electrocautery cable to the rabbit drape using the 7.25" Kantrowitz Forceps. Connect the plug to the electrosurgery unit and turn it on.
- Fill a 20 mL syringe with sterile saline. Use this saline as needed to keep the exposed tissue moist during the procedure.
- Place the paper drape over the rabbit and cut a hole in the drape over the surgical site on rabbit's neck. Clamp the corners of hole in place to the rabbit's skin with the towel clamps.
- Isolate common carotid arteries.
NOTE: 2x surgical loupes should be used for this part.- Cut the skin with an electrocautery along the midline extending approximately 7 – 9 cm cranially toward the mandible and clamp skin open with towel clamps.
NOTE: If harvest is only a few days after previous surgery, electrocautery is not needed. Just cut the sutures and gently pull open the incision from the previous surgery. - Make a short lateral cut through the fascia with an electrocautery at the caudal end. Then insert large scissors into the cut and bluntly dissect the fascia along the entire midline. Cut the dissected fascia down the midline with the electrocautery.
- With small dissecting scissors, dissect between the V-shaped muscles (sternocephalic muscle) and the sternohyoid muscle over the trachea, to isolate the common carotid arteries, starting on the right side.
- Dissect the right artery free from surrounding tissues from base of neck caudally to the crossing of the pharyngeal nerve cranially. Use surgical silicon loops to aid in retracting the artery during dissection.
- Repeat dissection on the left side (steps 5.2.3 – 5.2.4).
- With a 3-0 silk suture, ligate the common carotid artery cranial to the segment that was infused with the vector (use adventitial suture placed at first surgery to locate the cranial extent of vector infusion. Then ligate the carotid caudal to the repaired arteriotomy.
- Excise the carotid segment between the ligations, and flush the lumen with saline. Trim away excess adventitial tissue from the vessel and cut the carotid segment into smaller pieces for the different endpoint analyses (histology, DNA, ribonucleic acid (RNA), protein, explant culture, etc.).
- Inject 1 mL of Beuthanasia IV to euthanize, and confirm euthanasia of the rabbit.
- Cut the skin with an electrocautery along the midline extending approximately 7 – 9 cm cranially toward the mandible and clamp skin open with towel clamps.
- Dispose of anything that had contact with vector or was in the operative field, following appropriate biohazard and sharps waste protocols.
Representative Results
To implement this method with confidence, preliminary experiments are necessary to establish that the operator achieves efficient and reproducible gene transfer, with transgene expression primarily in luminal endothelial cells. In our experience, this is most easily assessed using a vector that expresses β-galactosidase. 5-bromo-4-chloro-3-indolyl-β-D-galactopyranoside (X-gal) staining of common carotid segments removed 3 days after vector infusion, as well as measurement of β-galactosidase mRNA (messenger RNA) with quantitative reverse transcription polymerase chain reaction (qRT-PCR), will reveal efficiency, reproducibility, and location of the transduced cells. For experiments that investigate the effects of transgene expression or measure the activity of cis-acting transcriptional elements, we typically measure transgene mRNA as an initial indication of level and reproducibility of gene transfer.
A new operator in our laboratory sought to establish proficiency with this method by transducing rabbit common carotid arteries with an adenoviral vector (2 x 1011 vp/mL) expressing a β-galactosidase transgene, driven by a cytomegalovirus (CMV) promoter. Transduced arteries were harvested 3 days later and were cut transversely into segments. Individual segments were then either cut open axially or left as intact rings. All of the segments were X-gal stained in microcentrifuge tubes. Segments that had been cut open axially were placed on a horizontal surface and the luminal surface maximally exposed, using pins as needed to prevent the segment from curling up. En face images of the luminal surfaces showed robust endothelial staining with X-gal (Figures 3A and 3B). Axial images of the luminal surfaces of intact carotid rings showed X-gal staining only on the luminal surface (Figures 3C and 3D). The segments that had been opened axially were processed into paraffin, sectioned, and counter-stained with either hematoxylin and eosin or nuclear fast red. Images show X-gal staining primarily in the endothelium, although there is a small amount of staining in the adventitial layer (Figures 3E and 3F). Transduction of adventitial cells could occur via leakage of vector through the arteriotomy site or by leakage via small branches proximal to the sites of side branch ligation.29
In a separate experiment, a new operator sought to establish proficiency in achieving reproducible levels of transgene expression, as a prelude to experiments aimed at investigating biological activities of the transgenes. Rabbit common carotid arteries were transduced with helper-dependent adenovirus (2 x 1011 vp/mL) containing either an apo A-I (HDAdApoAI) or IL-10 (HDAdIL10) transgene, both under control of a CMV promoter. Transduced arteries were harvested 3 days after transduction and cut transversely into segments. RNA was extracted from the vessel segments, and apo A-I and IL-10 mRNA expressions were quantified by qRT-PCR, with normalization to glyceraldehyde 3-phosphate dehydrogenase (GAPDH) mRNA in the same extracts (Figure 4). In HDAdIL10-transduced arteries, only 1 out of 6 arteries had a very low, but detectable apo A-I mRNA signal. Mean expression of apo A-I mRNA was 700-fold greater in the vessels transduced with HDAdApoAI than in vessels transduced with HDAdIL10. Low levels of endogenous IL-10 mRNA were detected in HDAdApoAI-transduced arteries, with mean expression increased 6-fold in HDAdIL10-transduced arteries. Of note, there is considerable intra- and inter-artery variability in transduction efficiency and transgene expression, as shown in Figures 3 and 4, respectively. We find this variability even with experienced operators.
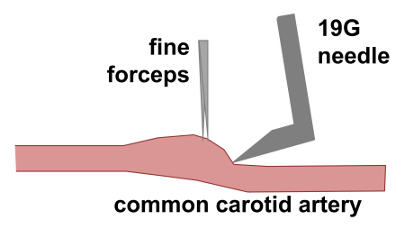
Figure 1. Arteriotomy in common carotid artery. Fine forceps are used to grasp the carotid artery adventitia and apply upward traction to the artery. This maneuver expands the vessel lumen and generates a vertical surface into which the bent 19G needle is inserted, thereby minimizing the risk of puncturing the back wall of the artery. Please click here to view a larger version of this figure.
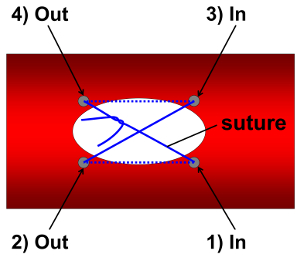
Figure 2. Closure of common carotid arteriotomy. The arteriotomy is closed with a 7-0 polypropylene suture, using an X-pattern. The first pass of the needle and suture enters the artery lumen at bottom right of the arteriotomy (site 1) and exits the lumen at the bottom left (site 2). The needle and suture then cross the arteriotomy and re-enter the lumen at the top right (site 3). The needle then exits the lumen at the top left (site 4). Gentle traction on both ends of the suture closes the arteriotomy. The suture ends (exiting from site 1 and site 4) are tied with 2 square knots. Grey circles represent sites of sutures passing through the vessel wall. Solid blue lines indicate areas where the suture is outside of the vessel wall. Dotted blue lines indicate areas where the suture is within the lumen. Please click here to view a larger version of this figure.
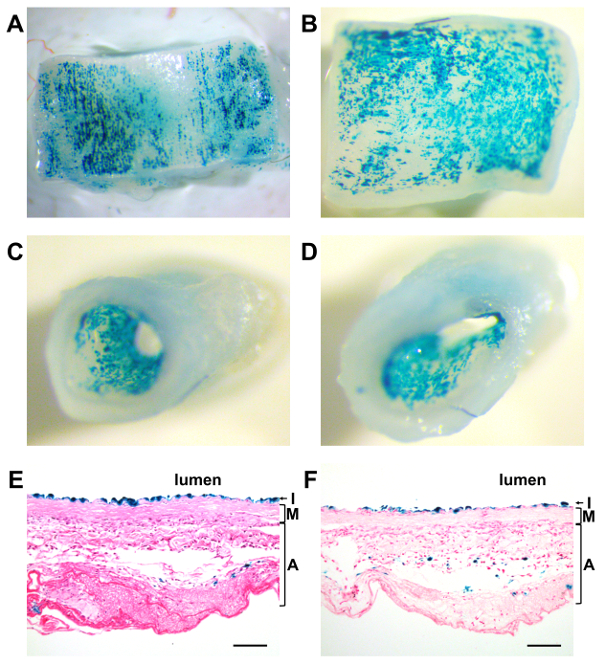
Figure 3. Efficient endothelial transgene expression. Rabbit common carotid arteries were transduced with an adenoviral vector expressing a β-galactosidase transgene and harvested 3 days later. Transduced artery segments were X-gal stained either as intact rings or after being opened with an axial cut. (A–B) En face images of the luminal surfaces of carotid rings that were cut open axially. (C–D) Axial views into the luminal space of intact carotid rings. (E–F) X-gal stained, paraffin-embedded carotid segments were sectioned and counter-stained with either (E) hematoxylin and eosin or (F) nuclear fast red. Scale bar = 100 µm. I = intima; M = media; and A = adventitia. Please click here to view a larger version of this figure.
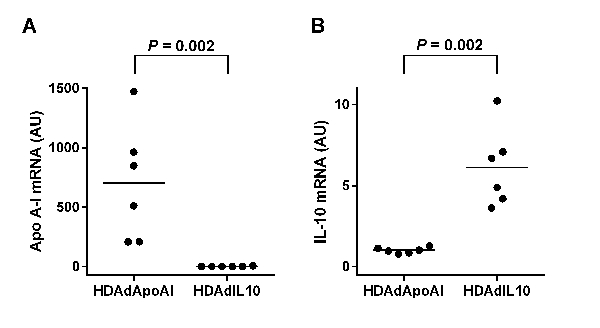
Figure 4. Quantification of transgene mRNA expression. Rabbit common carotid arteries were transduced with helper-dependent adenovirus expressing either apo A-I (HDAdApoAI) or IL-10 (HDAdIL10) under control of a CMV promoter. Arteries were harvested 3 days later. mRNA expression of (A) Apo A-I and (B) IL-10 were quantified by qRT-PCR, normalized to GAPDH mRNA in the same artery, and expressed as arbitrary units (AU). Bar indicates mean value; P value is from rank-sum test. Please click here to view a larger version of this figure.
| Advantages | Disadvantages | |
| Compared to Rodent Models | Closer phylogenetically to primates | More expensive to purchase and house |
| Greater genetic diversity, easing clinical translation | More difficult to breed and handle | |
| Larger vessels allow easier surgical manipulation and provides more tissue for quantitative analysis | More extensive regulatory requirements | |
| Allows use of endovascular devices designed for humans | Fewer genetically modified backgrounds | |
| Less-extensive selection of antibodies to rabbit proteins | ||
| Compared to Larger Animal Models | Relatively inexpensive to purchase and house | Possibly less clinically relevant than other large animal models for some vascular diseases |
| Easier to breed and handle | ||
| Compared to Germ-line Transgenesis | Transgene expressed only in large artery; effect of transgene specifically at site of interest can be determined | Application of method to cells other than endothelium is difficult |
| Can use contralateral carotid as a paired control; eliminates systemic parameters (e.g., blood pressure, cholesterol level) as uncontrolled variables | Operating room and surgical expertise required; core facilities likely not available | |
| Higher throughput for testing DNA regulatory sequence activity in large vessel endothelium | Transgene cannot be expressed in most vascular beds | |
| Potentially quicker and less expensive | ||
| Systemic exposure to transgenic protein unlikely —minimizes off-target effects | ||
| Compared to Systemic Gene Therapy Approaches (e.g,. Liver Transduction via Peripheral Vein injection) |
More-stable transgene expression than systemic (liver) gene therapy | Vector delivery requires surgical intervention |
| Transgene expressed in artery wall, allowing local delivery of high levels of transgenic protein | Operating room and surgical expertise required | |
| Systemic exposure to transgenic protein unlikely —minimizes off-target effects | Treatment limited to arteries that are specifically targeted for intervention; does not treat systemic factors (e.g., lipids) | |
| Can use contralateral carotid as a paired control; eliminates systemic parameters (e.g., blood pressure, cholesterol level) as uncontrolled variables | ||
| Far lower vector dose required |
Table 1. Advantages and disadvantages of rabbit common carotid artery endothelial-selective gene transfer model.
Discussion
Certain aspects of surgical technique merit particular attention. Full exposure and mobilization of the common carotid artery via careful dissection will facilitate gene transfer and arteriotomy repair. However, during the dissection, direct manipulation of the carotid artery should be minimized to prevent vasospasm. In addition, any bleeding adjacent to the artery should be stopped by applying light pressure with gauze and extravasated blood should be cleaned up immediately by rinsing the area with normal saline. It is also important to avoid damaging the vagus nerve, which runs parallel to the common carotid artery. Trimming the adventitia in the area of the planned arteriotomy will help the operator both to perform a clean and functional arteriotomy and to repair the arteriotomy. Finally, branches off the common carotid artery must be identified and securely ligated to prevent leakage of the vector from the carotid lumen.
There are also critical aspects of vector infusion and arteriotomy repair. During vector infusion, it is important to distend the common carotid to physiological or slightly greater caliber to achieve efficient transduction. When repairing the arteriotomy, the suture should penetrate the vessel wall as close as possible to the edges of the arteriotomy, and should cleanly enter and exit the lumen rather than pass axially through the vessel wall. If only the outer layers of the vessel wall are pulled together because the suture passes axially through the vessel wall rather than passing radially through the wall and entering the lumen, a gap will remain in the intima and the risk of thrombosis will increase. If the suture penetrations are too widely spaced, or if the suture is over-tightened when tied, tissue folds will be created at the arteriotomy site. These folds disrupt normal laminar blood flow, also increasing thrombosis risk. Maintaining consistent flow characteristics is important for experiments performed in animal models of diseases (e.g., atherosclerosis) because altered flow can contribute to the disease process30.
New operators often encounter thrombosed arteries at harvest. Luminal thrombosis is a devastating complication, rendering the artery unusable as an experimental sample. To prevent thrombosis, we routinely administer IV heparin before gene transfer. Thrombosis is also prevented by careful closure of the arteriotomy, as described above. The heparin dosage could be increased to prevent thrombosis, or aspirin could be given postoperatively. However, a higher dose of heparin would also increase the potential for bleeding complications, and aspirin could interfere with experimental end points, especially if inflammation is being studied. Therefore, it is preferable to focus on improved surgical technique as a means of preventing thrombosis.
If manipulated too vigorously, carotid arteries may undergo spasm, which could also contribute to thrombosis by decreasing flow. If vasospasm is encountered, it can be relieved by application of topical papaverine. When vessel harvests are planned for more than 2 – 3 days after transduction, and thrombosis is a concern, transcutaneous ultrasound can be used to noninvasively assess vessel patency. Discovery of thrombosed arteries may lead to euthanasia in order to save on housing costs. Additional animals can also be enrolled promptly, to fill experimental groups. Peri- and post-intervention mortality associated with this method should be <1% (i.e., not different from mortality associated with other surgeries performed on healthy rabbits)31.
After an operator becomes comfortable with the technical aspects of the surgical protocol, an ability to perform efficient gene transfer to the endothelium needs to be verified, using approaches described in the section above on representative results. If issues arise with achieving reproducible gene transfer, the culprit is likely in one of two areas. After the vessel is isolated and the blood is washed from the lumen, it is important to remove the DMEM wash buffer so that the infused vector solution is not diluted during transduction. The other important aspect is to distend the vessel to physiological or slightly greater caliber during vector infusion. Because, in our experience, a carotid artery that is not fully distended or does not remain distended during the 20-minute infusion reliably has low transgene expression, it is likely that distension of the artery to physiologic caliber improves the transduction efficiency. However, we have never studied this systematically. It is possible that increasing the infusion pressure above physiological levels could increase transduction efficiency, and also allow higher levels of transduction of cells in the vascular media. However, disruption of the endothelial barrier would likely damage the vessel and increase the risk of thrombosis. If the vessel does not remain distended for the entire 20-minute vector-incubation period, it is likely that the vector is leaking from branches of the common carotid artery. Be careful during dissection to identify and ligate all branches to prevent leakage of the vector from the carotid lumen.
This method has several limitations that are related to the use of rabbits. Rabbits are less expensive to house and feed than other large animals (dogs, pigs, sheep); however, the costs of purchasing, housing, and feeding rabbits are considerably more than for mice and rats. The operating room facilities and regulatory requirements for rabbit surgeries are also far more extensive than for rodents. In addition, considerable technical expertise is needed to perform the surgical gene transfer protocol effectively. This expertise can be acquired by operators who have had no formal surgical training. At least 2 individuals in our group (including the primary author of this manuscript) have learned the surgical techniques and applied them productively. Nevertheless, meticulous training and a careful validation of an operator's gene transfer efficiency and reproducibility (as described in the representative results section) are needed before the operator can begin to generate high-quality data.
Confinement of transgene expression almost exclusively to the endothelium with this method29,32,33,34,35,36,37 is useful in that it allows investigation of transgene effects in endothelial cells and measurement of activity of cis-acting DNA regulatory sequences in endothelial cells. A small number of adventitial or medial cells may be transduced; however, the inability of this method to efficiently transduce nonendothelial cells prevents the application of the method to the study of other types of vascular wall cells (such as smooth muscle cells and macrophages). Although overexpression of secreted proteins from transduced endothelial cells can allow investigation of effects of these proteins on other vascular cell types, the roles of non-secreted proteins in these other vascular cell types (e.g. receptors or proteins involved in signal transduction) cannot be investigated with this method.
As a means for testing artery wall-targeted gene therapy, the method differs from other preclinical methods in two major ways. First, the method utilizes a rabbit model for in vivo testing of gene therapy rather than more commonly used rodent models8,12,15,38,39. The use of rabbits allows assessment of transgene expression and the biological role of the transgene product in an outbred animal model, which is more representative of human genetic diversity than are inbred rodents. The model can be used to assess gene therapy in either normal rabbit arteries or in rabbit arteries that have arterial pathology that is similar to that found in diseased human arteries. Rabbit arteries also are closer in size to human arteries than are rodent arteries and provide far more tissue for analysis than is available from rodent arteries. The second major difference is that this method uses a surgical approach to deliver transgene vector to the vascular endothelium. Somatic gene therapy is often delivered systemically, most frequently by targeting the liver with the goal of altering plasma levels of the transgene protein25,40. By targeting vascular endothelium, the method supplies the therapeutic transgene product locally, with its peak concentration within the artery wall, precisely where it is needed for vascular disease treatment. By delivering the transgene only locally, the method also eliminates systemic side effects of the transgene product. Other groups are developing methods using peptides, antibodies, or other capsid modifications for targeting systemically injected vectors to healthy or diseased endothelium to provide local vascular gene therapy41,42,43. However, these targeting methods remain under development, and are still complicated by substantial systemic transduction, especially in the liver42,43,44. Our surgical method provides a precise and efficient introduction of transgenes to the vascular endothelium with minimal – if any – transduction at other locations.1 The method is also a more convenient, efficient, and higher-throughout mean (compared to germ-line transgenesis or systemic injection of endothelial-targeted vectors) for testing the activity of DNA regulatory sequences in the large vessel endothelium, for testing transgene protein function in the artery wall, and for testing vessel-wall-targeted gene therapy.
This method allows investigation of the biological role of any transgene, when it is expressed in the large artery endothelium. If modified to express loss-of-function reagents such as dominant negative receptors or short hairpin RNA, it would permit investigation of the roles of endogenous endothelial proteins and signaling pathways. The method can also be used to measure the transcriptional activity of any cis-acting DNA sequence in large artery endothelial cells5,6,7. In addition, the method allows testing of any type of gene transfer vector for efficiency and safety when delivered locally to endothelium, and will reveal the ability of the vector to achieve durable transgene expression. Finally, the method allows development and testing of combinations of vectors and transgenes that are designed to deliver vascular wall-targeted gene therapy. The method could serve as a screening tool to identify therapeutic genes that might-in the future-be delivered to the endothelium of all large arteries (or all diseased large arteries) by percutaneously injected vascular wall-targeted vectors. Because of pre-existing immunity in humans to adenovirus type 545, it will be challenging to use adenovirus type 5-based vectors in clinical applications. Engineering of the adenovirus 5 capsid, use of alternative adenovirus serotypes46, or use of less-immunogenic vectors such as AAV may be required to bring vascular gene therapy to the clinic. As an experimental tool, however, we are unaware of any vector that can compete with helper-dependent adenovirus 5 in achieving efficient and durable transgene expression in blood vessels1.
Disclosures
The authors have nothing to disclose.
Acknowledgements
We thank AdVec, Inc. for permission to use HDAd reagents, Julia Feyk for administrative assistance, and the Department of Comparative Medicine veterinary services for surgical advice and support. This work was supported by HL114541 and the John L. Locke, Jr. Charitable Trust.
Materials
| Disposables | |||
| 3mL syringe with 24G needle | Becton Dickinson | 309571 | 2x for gene transfer surgery; 3x for harvest surgery |
| 1mL syringe with 27G needle | Becton Dickinson | 309623 | 6x for gene transfer surgery; 1x for harvest surgery |
| 20mL syringe, luer lock | Nipro Medical Corp | JD+20L | |
| Catheters, 24G x 3/4" | Terumo Medical Products | SROX2419V | |
| 19G needle | Becton Dickinson | 305187 | Gene transfer surgery only |
| 21G needle | Becton Dickinson | 305165 | For 20 mL syringe of saline |
| Gauze 4" x 4" | Dynarex | 3242 | ~10-15 per surgery |
| 3-0 silk suture | Covidien Ltd. | S-244 | |
| 5-0 silk suture | Covidien Ltd. | S-182 | Gene transfer surgery only |
| 7-0 polypropylene suture | CP Medical | 8648P | Gene transfer surgery only |
| 5-0 polyglycolic acid suture | CP Medical | 421A | Gene transfer surgery only |
| 3-0 polyglycolic acid suture | CP Medical | 398A | Gene transfer surgery only |
| Alcohol swabs | Covidien Ltd. | 6818 | For placement of I.V. line |
| Catheter plug | Vetoquinol | 411498 | Gene transfer surgery only |
| Ketamine HCl, 100 mg/mL | Vedco Inc. | 05098916106 | |
| Xylazine, 100 mg/mL | Akorn Inc. | 4821 | |
| Lidocaine HCl, 2% | Pfizer | 00409427702 | |
| Bupivacaine HCl, 0.5% | Pfizer | 00409161050 | |
| Beuthanasia D-Special | Intervet Inc. | NDC 00061047305 | Harvest surgery only |
| Buprenorphine HCl, 0.3 mg/mL | Patterson Veterinary | 12496075705 | Gene transfer surgery only |
| Saline IV bag, 0.9% sodium chloride | Baxter | 2B1309 | 2x for gene transfer surgery; can use vial of sterile saline in place of one |
| Heparin (5000 U/mL) | APP Pharmaceuticals | NDC 63323-047-10 | Gene transfer surgery only |
| Fentanyl patch, 25 mcg/hr | Apotex Corp. | NDC 60505-7006-2 | Gene transfer surgery only |
| Isoflurane | Multiple vendors | Catalog number not available | |
| Gene transfer vector | Dilute 350 µL per artery; 2 x 1011 vp/mL for adenovirus; gene transfer surgery only | ||
| Surgical Instruments | |||
| Metzenbaum needle holder 7" straight | Roboz | RS-7900 | Gene transfer surgery only |
| Operating scissors 6.5" straight blunt/blunt | Roboz | RS-6828 | |
| Needle holder /w suture scissors | Miltex | 8-14-IMC | Gene transfer surgery only |
| Castroviejo scissors | Roboz | RS-5658 | |
| Castroviejo needle holder, 5.75" straight with lock | Roboz | RS-6412 | Gene transfer surgery only |
| Stevens scissors 4.25" curved blunt/blunt | Roboz | RS-5943 | |
| Alm retractor 4" 4X4 5mm blunt prongs | Roboz | RS-6514 | 2x |
| Backhaus towel clamp 3.5" | Roboz | 4x | |
| Micro clip setting forceps 4.75" | Roboz | RS-6496 | Gene transfer surgery only |
| Micro vascular clips, 11 mm | Roboz | 2x for gene transfer surgery only | |
| Surg-I-Loop | Scanlan International | 1001-81M | 5 cm length |
| Bonaccolto forceps, 4” (10 cm) long longitudinal serrations, cross serrated tip, 1.2mm tip width | Roboz | RS-5210 | |
| Dumont #3 forceps Inox tip size .17 X .10mm | Roboz | RS-5042 | |
| Graefe forceps, 4” (10 cm) long serrated straight, 0.8mm tip | Roboz | RS-5280 | |
| Halstead mosquito forceps, 5" straight, 1.3mm tips | Roboz | RS-7110 | 2x |
| Halstead mosquito forceps, 5" curved, 1.3mm tips | Roboz | RS-7111 | |
| Jacobson mosquito forceps 5" curved extra delicate, 0.9 mm tips | Roboz | RS-7117 | |
| Kantrowitz forceps, 7.25" 90 degree delicate, 1.7 mm tips | Roboz | RS-7305 | |
| Tissue forceps 5", 1X2 teeth, 2 mm tip width | Roboz | RS-8162 | |
| Allis-Baby forceps, 12 cm, 4×5 teeth, 3 mm tip width | Fine Science Tools | 11092-12 | 2x |
| Adson forceps, 12 cm, serrated, straight | Fine Science Tools | 11006-12 | |
| Veterinary electrosurgery handpiece and electrode | MACAN Manufacturing | HPAC-1; R-F11 | |
| Surgical Suite Equipment | |||
| Circulating warm water blanket and pump | Multiple vendors | Catalog number not available | |
| Forced air warming unit | 3M | Bair Hugger Model 505 | Gene transfer surgery only |
| IV infusion pump | Heska | Vet IV 2.2 | Gene transfer surgery only |
| Isoflurane vaporizer and scavenger | Multiple vendors | Catalog number not available | |
| Veterinary multi-parameter monitor | Surgivet | Surgivet Advisor | |
| Veterinary electrosurgery unit | MACAN Manufacturing | MV-9 | |
| Surgical microscope | D.F. Vasconcellos | M900 | Needs ~16x magnification |
References
- Flynn, R., et al. Expression of apolipoprotein A-I in rabbit carotid endothelium protects against atherosclerosis. Mol Ther. 19, 1833-1841 (2011).
- Falkenberg, M., et al. Increased expression of urokinase during atherosclerotic lesion development causes arterial constriction and lumen loss, and accelerates lesion growth. Proc Natl Acad Sci U S A. 99, 10665-10670 (2002).
- Schneider, D. B., et al. Expression of Fas ligand in arteries of hypercholesterolemic rabbits accelerates atherosclerotic lesion formation. Arterioscler Thromb Vasc Biol. 20, 298-308 (2000).
- Du, L., Dronadula, N., Tanaka, S., Dichek, D. A. Helper-dependent adenoviral vector achieves prolonged, stable expression of interleukin-10 in rabbit carotid arteries but does not limit early atherogenesis. Hum Gene Ther. 22, 959-968 (2011).
- Dronadula, N., et al. Construction of a novel expression cassette for increasing transgene expression in vivo in endothelial cells of large blood vessels. Gene Ther. 18, 501-508 (2011).
- Dronadula, N., Wacker, B. K., Van Der Kwast, R., Zhang, J., Dichek, D. A. Stable In Vivo Transgene Expression in Endothelial Cells with Helper-Dependent Adenovirus: Roles of Promoter and Interleukin-10. Hum Gene Ther. 28, 255-270 (2017).
- Dong, G., Schulick, A. H., DeYoung, M. B., Dichek, D. A. Identification of a cis-acting sequence in the human plasminogen activator inhibitor type-1 gene that mediates transforming growth factor-b1 responsiveness in endothelium in vivo. J Biol Chem. 271, 29969-29977 (1996).
- Byrom, M. J., Bannon, P. G., White, G. H., Ng, M. K. Animal models for the assessment of novel vascular conduits. J Vasc Surg. 52, 176-195 (2010).
- Zeng, Z., et al. Hemodynamics and anatomy of elastase-induced rabbit aneurysm models: similarity to human cerebral aneurysms. AJNR Am J Neuroradiol. 32, 595-601 (2011).
- Macdonald, R. L., Wallace, M. C., Montanera, W. J., Glen, J. A. Pathological effects of angioplasty on vasospastic carotid arteries in a rabbit model. J Neurosurg. 83, 111-117 (1995).
- Nakai, K., Numaguchi, Y., Moritani, T. Vasospasm model of a rabbit common carotid artery for endovascular research. Acad Radiol. 9, 270-275 (2002).
- Zaragoza, C., et al. Animal models of cardiovascular diseases. J Biomed Biotechnol. 2011, 497841 (2011).
- Baumgartner, C., Brandl, J., Munch, G., Ungerer, M. Rabbit models to study atherosclerosis and its complications – Transgenic vascular protein expression in vivo. Prog Biophys Mol Biol. 121 (2), 131-141 (2016).
- Wang, K., et al. Three-Layered PCL Grafts Promoted Vascular Regeneration in a Rabbit Carotid Artery Model. Macromol Biosci. 16 (4), 608-618 (2016).
- Schachner, T., Laufer, G., Bonatti, J. In vivo (animal) models of vein graft disease. Eur J Cardiothorac Surg. 30, 451-463 (2006).
- Dornas, W. C., Oliveira, T. T., Augusto, L. E., Nagem, T. J. Experimental atherosclerosis in rabbits. Arq Bras Cardiol. 95 (2), 272-278 (2010).
- Graur, D., Duret, L., Gouy, M. Phylogenetic position of the order Lagomorpha (rabbits, hares and allies). Nature. 379 (6563), 333-335 (1996).
- Yanni, A. E. The laboratory rabbit: an animal model of atherosclerosis research. Lab Anim. 38, 246-256 (2004).
- Miao, C. H., et al. Inclusion of the hepatic locus control region, an intron, and untranslated region increases and stabilizes hepatic factor IX gene expression in vivo but not in vitro. Mol. Ther. 1, 522-532 (2000).
- Wen, S., Graf, S., Massey, P. G., Dichek, D. A. Improved vascular gene transfer with a helper-dependent adenoviral vector. Circulation. 110, 1484-1491 (2004).
- Schlaeger, T. M., et al. Uniform vascular-endothelial-cell-specific gene expression in both embryonic and adult transgenic mice. Proc Natl Acad Sci U S A. 94 (7), 3058-3063 (1997).
- Cowan, P. J., et al. Targeting gene expression to endothelial cells in transgenic mice using the human intercellular adhesion molecule 2 promoter. Transplantation. 62 (2), 155-160 (1996).
- Sehara, Y., et al. Persistent Expression of Dopamine-Synthesizing Enzymes 15 Years After Gene Transfer in a Primate Model of Parkinson’s Disease. Hum Gene Ther Clin Dev. 28, 74-79 (2017).
- Tangirala, R. K., et al. Regression of atherosclerosis induced by liver-directed gene transfer of apolipoprotein A-I in mice. Circulation. 100, 1816-1822 (1999).
- Benoit, P., et al. Somatic gene transfer of human ApoA-I inhibits atherosclerosis progression in mouse models. Circulation. 99, 105-110 (1999).
- Raper, S. E., et al. Fatal systemic inflammatory response syndrome in a ornithine transcarbamylase deficient patient following adenoviral gene transfer. Mol Genet Metab. 80, 148-158 (2003).
- Wacker, B. K., Dronadula, N., Zhang, J., Dichek, D. A. Local Vascular Gene Therapy With Apolipoprotein A-I to Promote Regression of Atherosclerosis. Arterioscler Thromb Vasc Biol. 37, 316-327 (2017).
- Brunetti-Pierri, N., et al. Transgene expression up to 7 years in nonhuman primates following hepatic transduction with helper-dependent adenoviral vectors. Hum Gene Ther. 24, 761-765 (2013).
- Rome, J. J., et al. Anatomic barriers influence the distribution of in vivo. gene transfer into the arterial wall. Modeling with microscopic tracer particles and verification with a recombinant adenoviral vector. Arterioscler Thromb. 14, 148-161 (1994).
- Cunningham, K. S., Gotlieb, A. I. The role of shear stress in the pathogenesis of atherosclerosis. Lab Invest. 85, 9-23 (2005).
- Brodbelt, D. Perioperative mortality in small animal anaesthesia. Vet J. 182, 152-161 (2009).
- Schulick, A. H., Dong, G., Newman, K. D., Virmani, R., Dichek, D. A. Endothelium-specific in vivo gene transfer. Circ Res. 77, 475-485 (1995).
- Vassalli, G., Agah, R., Qiao, R., Aguilar, C., Dichek, D. A. A mouse model of arterial gene transfer. Antigen-specific immunity is a minor determinant of the early loss of adenovirus-mediated transgene expression. Circ Res. 85, 25-32 (1999).
- Schneider, D. B., Fly, C. A., Dichek, D. A., Geary, R. L. Adenoviral gene transfer in arteries of hypercholesterolemic nonhuman primates. Hum Gene Ther. 9, 815-821 (1998).
- Newman, K. D., et al. Adenovirus-mediated gene transfer into normal rabbit arteries results in prolonged vascular cell activation, inflammation, and neointimal hyperplasia. J Clin Invest. 96, 2955-2965 (1995).
- Jiang, B., et al. Helper-dependent adenovirus is superior to first-generation adenovirus for expressing transgenes in atherosclerosis-prone arteries. Arterioscler Thromb Vasc Biol. 31, 1317-1325 (2011).
- Gruchala, M., et al. Gene transfer into rabbit arteries with adeno-associated virus and adenovirus vectors. J Gene Med. 6, 545-554 (2004).
- Lee, Y. T., et al. Mouse models of atherosclerosis: a historical perspective and recent advances. Lipids Health Dis. 16, 12 (2017).
- Manning, M. W., Cassi, L. A., Huang, J., Szilvassy, S. J., Daugherty, A. Abdominal aortic aneurysms: fresh insights from a novel animal model of the disease. Vasc Med. 7, 45-54 (2002).
- Lai, C. H., et al. Recombinant adeno-associated virus vector carrying the thrombomodulin lectin-like domain for the treatment of abdominal aortic aneurysm. Atherosclerosis. 262, 62-70 (2017).
- Tan, P. H., et al. Antibody targeted gene transfer to endothelium. J Gene Med. 5, 311-323 (2003).
- Nicklin, S. A., White, S. J., Nicol, C. G., Von Seggern, D. J., Baker, A. H. In vitro and in vivo characterisation of endothelial cell selective adenoviral vectors. J Gene Med. 6, 300-308 (2004).
- White, K., et al. Engineering adeno-associated virus 2 vectors for targeted gene delivery to atherosclerotic lesions. Gene Ther. 15, 443-451 (2008).
- Kaliberov, S. A., et al. Retargeting of gene expression using endothelium specific hexon modified adenoviral vector. Virology. 447, 312-325 (2013).
- Schulick, A. H., et al. Established immunity precludes adenovirus-mediated gene transfer in rat carotid arteries. Potential for immunosuppression and vector engineering to overcome barriers of immunity. J Clin Invest. 99, 209-219 (1997).
- Hollingdale, M. R., Sedegah, M., Limbach, K. Development of replication-deficient adenovirus malaria vaccines. Expert Rev Vaccines. 16, 261-271 (2017).
