Successful LDPI should result in consistent repeated measures scans, with no more than 100-150 perfusion unit variation (corresponding to about 10% of the usual mean perfusion for the mouse footpad) between the three scans (Figure 2). As demonstrated in Figure 2, repeat scans help determine that the mouse has been appropriately equilibrated so that the ischemic/control ratio best reflects the underlying blood flow as opposed to variation in dermal perfusion caused by temperature variation. Using single scans for datapoints will increase the variability leading to the need for more experimental mice. When used for hindlimb ischemia, the surgical hindlimb should have decreased global perfusion when compared to the control hindlimb. Results are expressed as a ratio of surgical hindlimb perfusion/control hindlimb perfusion. As mice initially vasodilate and develop their intrinsic collateral network over time, blood flow recovery by LDPI should be seen over a postoperative time course (Figure 4). The degree of recovery is dependent on the mouse strain and severity of the hindlimb ischemia model.
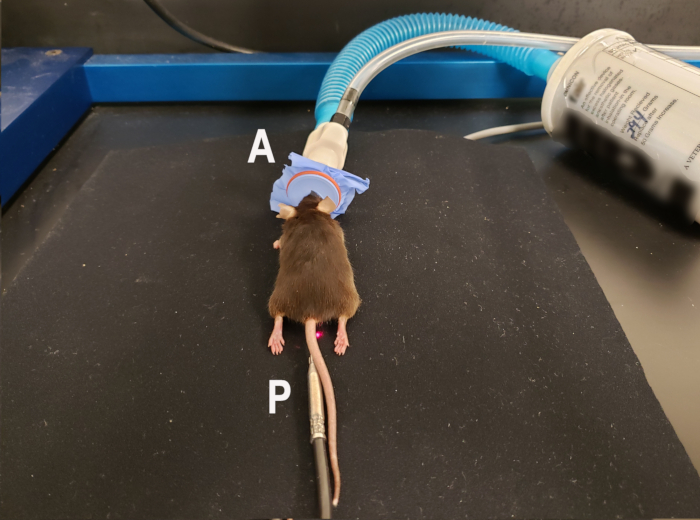
Figure 1. Mouse positioning for laser Doppler perfusion imaging of the ventral footpads. Anesthetized mouse using isoflurane nose cone (A) is placed in the prone position with hindlimbs extended to allow scanning of the ventral footpads. Rectal temperature probe (P) for homeothermic blanket is in place to maintain consistent body temperature during the scan. The homeothermic blanket pad is underneath the nonreflective neoprene material used to provide background for the scan. Laser indicating the middle of the scanning region is visible next to the mouse's tail. Please click here to view a larger version of this figure.
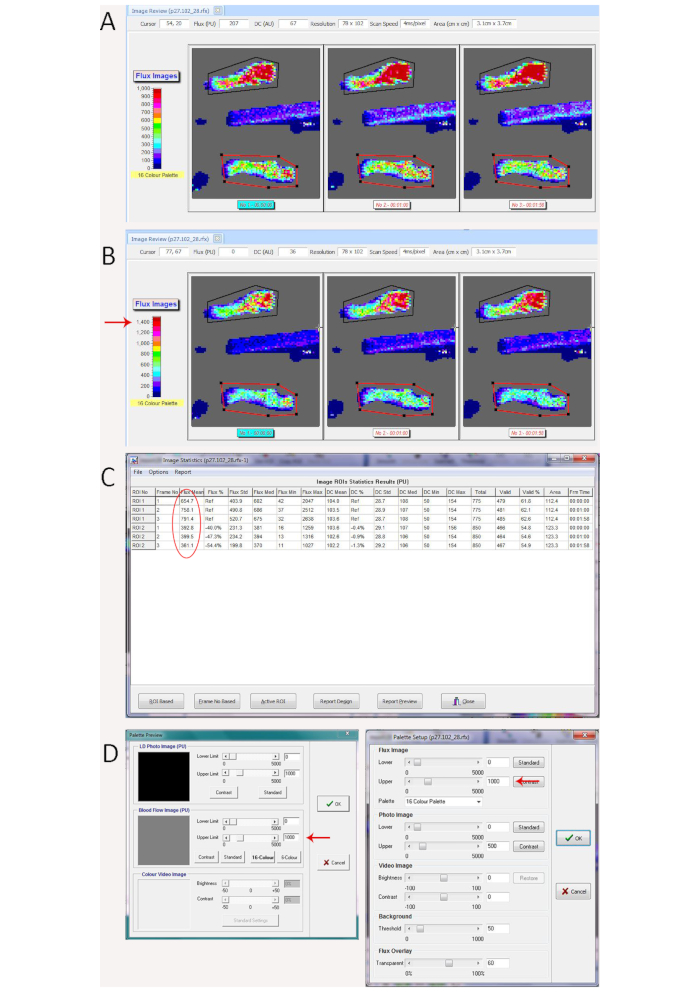
Figure 2. Demonstration of scan variation from mouse temperature change better seen with color palette adjustment. (A) Laser Doppler repeated scans with significant variation caused by mouse core temperature variation during the repeated scans, which is visible based on the perfusion units translated to color on the repeated flux scans. (B) Changing the dynamic range on the color palette (shown on the left of the scan window) from 0-1000 in A to 0-1500 (red arrow) in B makes the variation more obvious. (C) Statistics showing mean perfusion values for the region of interest (circled in red) for the control hindlimb (Polygon 1 in black on the rfx image in A and B) ranges between 655 for the 1st scan to 791 on the 3rd scan and mean perfusion for the region of interest for the ischemic hindlimb (Polygon 2 in red on the rfx image in A and B) showed less variation (361 to 400), leading to significant differences in the ischemic/control ratio between the repeated scans (0.60, 0.53, and 0.46). (D) Window to change the dynamic range of the color palette in the measurement software (left panel) and image review software (right panel). Red arrows show where to increase or decrease the upper range. Please click here to view a larger version of this figure.
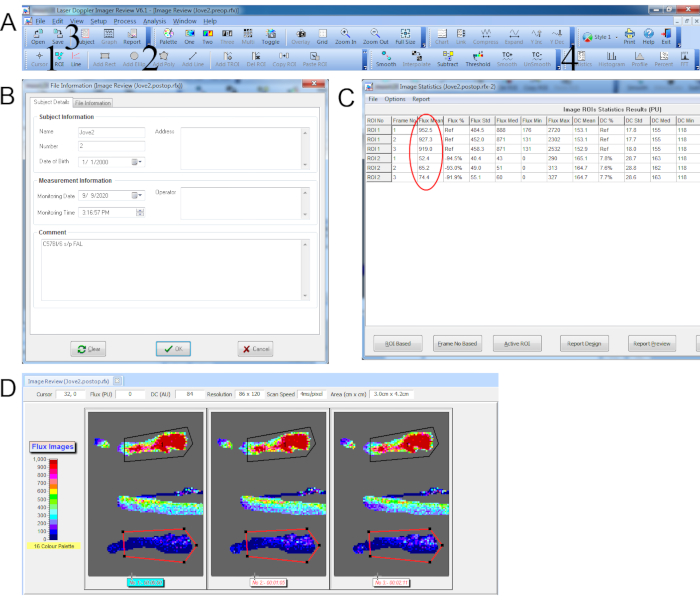
Figure 3. Data capture for laser Doppler perfusion imaging with repeated scans. (A) Top toolbar with 1. Add ROI icon. 2. Add Polygon icon. 3. Subject details icon (accesses window pop-up in B). 4. Statistics icon (accesses window pop-up in C). (B) Subject details window. (C) Statistics window showing the mean perfusion values (circled in red) for each ROI. (D) Repeated scan with polygon ROI traced around control hindpaw (black) and ischemic hindpaw (red). Please click here to view a larger version of this figure.
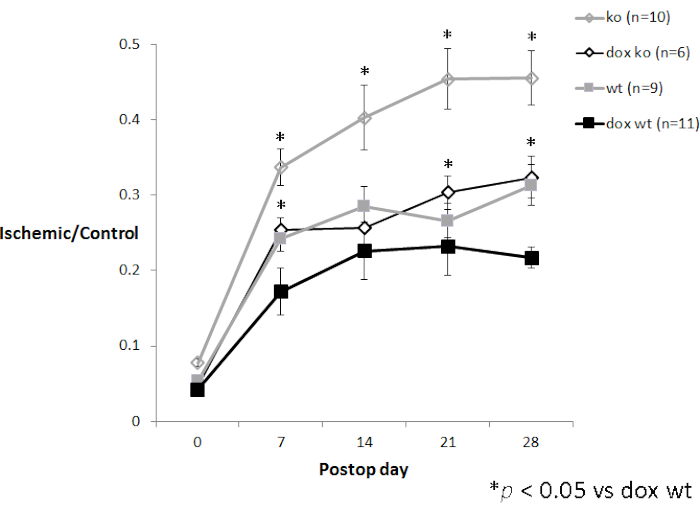
Figure 4. Time course experiment with LDPI data. P27 knockout mice (3-5 month old female CDKN1b-/- mice on a C57Bl/6 background) after femoral artery ligation with (n=6) and without (n=10) oral doxycycline treatment compared to age-matched female wildtype C57Bl/6 mice with (n=11) and without (n=9) oral doxycycline treatment (unpublished data from the author). Error bars represent standard error of the mean (SEM). Please click here to view a larger version of this figure.
