Fabrication of the C-seal
The C-Seal is made of biodegradable polyurethane, composed of hard and soft molecular components. The hard component provides the material the desirable elastic and mechanical properties. The hard component consists of polyurethane bindings (HNCO2) composed of a di-isocyanate (OCN-NCO) and a diol (HO-OH).
The soft segment determines the degradation behavior of the polyurethane. The soft segment is called the prepolymer and consists of polyether-ester chains. The hard segment is incorporated into the soft segment. This incorporation is called ‘chain-extension’ of the polymerization.
Once these two segments interact, a poly-ether-ester-urethane is synthesized and the polymer is ready to be processed into a C-Seal:
- The polymer is diluted to a concentration suitable for spray coating.
- The polyurethane solution is sprayed on a rotating mould to a certain thickness.
- The mould is placed into a water bath in order to release the C-seal safely from the mould without causing damage.
- The C-seal is dried.
- The C-Seal is packaged in a Tyvek pouch and sterilized using EtO gas.
- After sterilization, the C-Seal is ready for use.
Surgical Procedure
The patient has given informed consent for participation in the C-seal study.
- The patient is positioned in the supine position in stirrups, the abdomen and perineum is disinfected and the patient is covered with sterile drapes.
- Establishment of pneumoperitoneum or laparotomy via midline incision.
- Inspection of the liver and abdominal cavity.
- Mobilization of the sigmoid colon and mobilization of the splenic flexure.
- In open surgery: division of the sigmoid colon at the level of the proximal resection margin.
- Right paramedian incision of the peritoneum, opening of the presacral plane; ligation and division of the superior rectal artery and vein.
- Mobilization of the mesorectum.
- Division of the rectum distally.
- In a laparoscopic setting: a suprapubic incision is performed to extract the specimen. Division of the proximal sigmoid colon.
- The C-seal can be used if the length of the rectal stump is max. 15 centimeters.
- The bowel diameter determines the stapler diameter; we prefer to use a CEA stapler with a diameter of 29 or 33 mm.
- The C-seal and a sterilized 12mm stainless steel marble are unpacked on a clean and sterile surface using clean and sterile surgical gloves.
- Open the C-seal, insert the marble and insert the anvil with the connection pin first. The two flaps in the opening of the C-seal are attached to the anvil using the two strips of adhesive tape.
- The anvil is advanced in the C-seal so that the connection pin ‘punctures’ the open pointed end of the C-seal. Gently unfold the C-seal completely and make sure the marble ends up inside the C-seal away from the anvil.
- Any type of anastomosis (end-to-end, end-to-side, side-to-end and side-to-side) can be performed when using the C-seal; we prefer to create a side-to-end anastomosis. There are multiple strategies to insert the anvil in the proximal bowel loop. The C-seal does not interfere with any of these strategies (open bowel end with pursestring suture/longitudinal bowel incision)
- Insert the anvil together with the C-seal in de proximal bowel loop by first advancing the C-seal with help of the marble and, if necessary, a blunt forceps. Ensure the tail of the C-seal is placed upwards in the bowel and check that the tail of the C-seal is stretched; check the position of the marble (the marble should be at adequate distance of the anvil). Then penetrate the bowel wall with the anvil’s pin and create a pursestring suture around the pin.
- Gently dilate the anus and insert the stapler in the rectal stump. Connect the anvil with the stapler. Check for torsion of the bowel.
- Fire the circular stapler. Now, the bowel ends are connected and the C-seal is attached to the staples
- Gently pull the stapler out of the anus. Do not turn the stapler more than 180 degrees when pulling out (the C-seal may twist). By removing the stapler from the rectum, the C-seal is pulled through the anus. Cut the C-seal at a distance of approximately 4 cm from the anus.
- Remove the marble from the rectum. Often the marble comes out together with the C-seal. If not, gently manually remove the marble which is situated between the C-seal and the intestinal wall.
- Verify the anastomosis. Optionally, perform an air-test by filling the pelvis with a saline solution and inject air into the anal canal (within the C-seal and between the C-seal and bowel). The absence of bubbles confirms a complete anastomosis.
- If indicated, create a protective stoma.
- In a laparoscopic setting: exsufflation of the abdominal cavity and trocars extraction.
- Close the incision(s)
- Postoperative phase:
Postoperative recovery is according to the ERAS (enhanced recovery after surgery) protocol9. The C-seal should be left in situ for at least one week. The patient has no restrictions and can lose stool via the C-seal. When the patient has recovered well and no anastomotic complications are suspected, the C-seal may be cut at the level of the anus. The remaining C-seal will degrade and the patient will lose the C-seal together with the stool via the natural route.
Representative Results
When the C-seal is applied correctly (figure 2 and 3), it covers the anastomosis. If a dehiscence is formed at the anastomotic site or distal from the anastomosis in the proximal rectal stump, extravasation of feces is prevented since the C-seal covers the defect and directs the fecal matter through the anus. In the postoperative phase, the C-seal protrudes from the anus (figure 3).
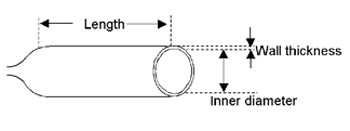
Figure 1: Schematic drawing of the C-seal.
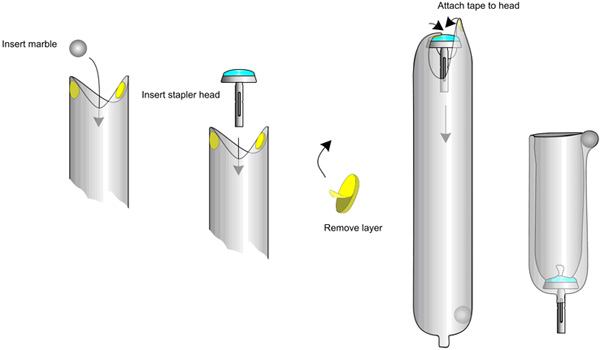
Figure 2: Schematic representation of attaching the C-seal to the stapler head.

Figure 3: After inserting the stapler-head together with the attached C-seal in the proximal bowel and the stapler in the rectal stump, the stapler is fired and gently pulled through the anus together with the C-seal.
